Conflation of biological sex and gender identity is at the root of the conflation of intersex and transgender. This conflation is based on the assumption that being transgender must be an “intersex condition of the brain”. However, while there is no scientific evidence of biological basis for gender identity, Disorders of Sex Development (formerly known as “intersex”) are well established in medicine and can be diagnosed using medical investigations, such as ultrasounds, chromosome testing or even simple physical examination. It is therefore unfortunate that this conflation worked so well that in 2020, international sporting authorities are using the rules designed to regulate participation of DSD (“intersex”) athletes in women’s sport, to allow fully sexed males who declare “female gender identity”, to compete in a female category.
Several high profile athletes already spoke out against the unfairness and compromised safety of female athletes under such rules. Others have remained silent for the fear of losing sponsorships and their place on the team. Scientists such as Dr Emma Hilton revieved available evidence and confirmed that male sporting advantage is significant and cannot be removed by testosterone suppression.

Why then, despite this science being available to all sporting authorities, do women and girls continue to be robbed of their records, wins and scholarships, by males who typically have a history of mediocre success while competing with other males, but find themselves dominating female competition with hardly any effort? And more alarmingly, why hasn’t this practice been stopped despite women suffering serious injuries, such as broken bones and fractured skulls, during sporting encounters with males?
World Rugby has thankfully committed to maintaining single-sex competitions in order to safeguard female athletes, but for this they have been pilloried by misogynists and gender activists alike, who maintain that “inclusiveness” is all important and to hell with the consequences for women and girls. The culture war is reaching a fever pitch, and considering the paralysis of institutions who should be leading the way back to evidence-based practices, maybe it is for the best that we’re in the middle of a pandemic. With sporting events suspended, at least more women and girl athletes aren’t being physically hurt and unfairly disadvantaged due to their female sex. But this temporary reprieve won’t last forever and unless something is done to reverse these dangerous and unfair rules, we are facing obliteration of women’s sport.
It is common knowledge that sport is segregated by biological sex due to males having sporting advantage over females (10-50% depending on sport) and that without this segregation, there can be no fair play for women and girls. It may therefore come as a surprise that in elite female athletics, the number of intersex competitors is already 140 times higher than in the normal female population. All these competitors are biological males. So as unpalatable and non-PC as it might be to say it, I feel inclusion of males in women’s sport is an issue more deeply entrenched than many realise.
In order to determine sex, biologists focus on the mechanics and look at whether the body developed down the pathway designed to produce large gametes called ova (typical human female, 46 XX) or small gametes called sperm (typical human male, 46 XY). Because we all develop from a single cell following fertilisation, many structures in our body start from a common precursor tissue which is then acted upon by different genes and enzymes to signal in which direction development of organ systems will take place. Disorders of sex development (DSDs or intersex) occur when something goes wrong and our bodies recieve erroneous signals, or fail to receive the right ones, and our development proceeds down the wrong pathway. However, because our genetic template is still either male or female, these anomalies can only impair that template, they cannot switch a male into a female or vice versa, and nowhere is this more apparent than in DSDs.
Some people believe that DSDs, as well as atypical karyotypes such as Kleinfelter’s XXY syndrome, produce a “variety of sexes” or a “sex spectrum” – they do not. Biological sex entails capacity for reproduction and for the most part, people with DSDs are infertile. And if they are fertile, they are so as their biological sex.
For example, in the cases of persistent Müllerian duct syndrome (PMDS), which is a male DSD, the Müllerian duct doesn’t regress, thanks to the absence of anti-müllerian hormone or its receptor. Males with this condition develop various abnormalities that affect their male reproductive organs as well as cause them to develop rudimentary female reproductive organs, such as a uterus or ovaries, which are non-functional and carry various health risks.
In Kleinfelter’s syndrome, which is not a DSD but rather an atypical male karyotype, the extra X chromosome leads to shortage of testosterone, so the male body fails to properly masculinise. And they can suffer with gynaecomastia ie. enlargement of male breast tissue, which might be superficially indistinguishable from a female breast but it doesn’t have the anatomy of the female breast, nor the function.

There are male DSDs, such as complete or partial AIS, that cause insensitivity to the effects of testosterone. This results in largely female appearance but internally, reproductive anatomy is still male.

In even rarer cases, certain genes from the Y chromosome transpose onto an X, so a 46XX DSD female embryo receives instruction to develop down the male pathway. But they are still biologically female, because they lack all the rest of the genes on the Y.
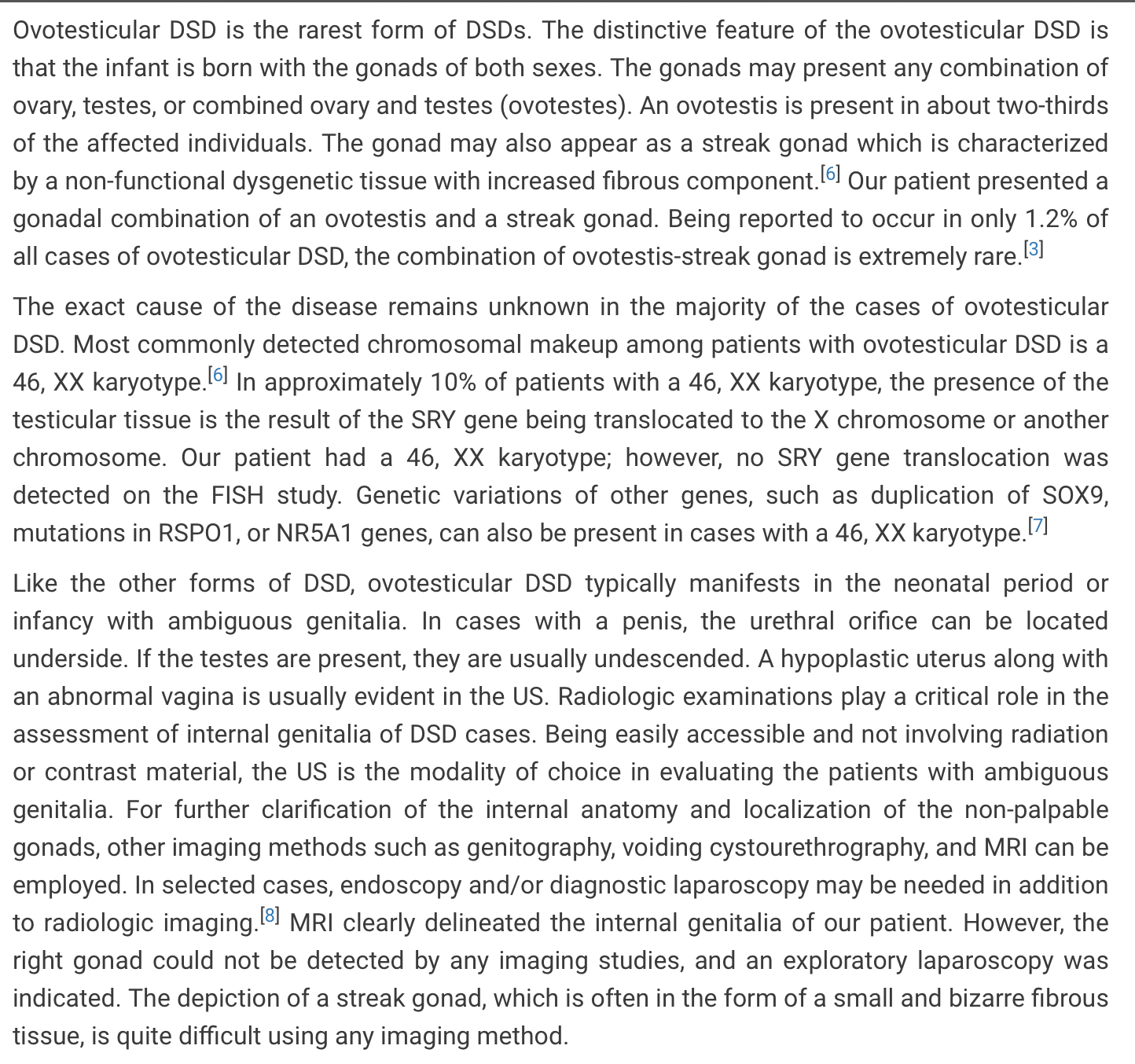
 And even in the case of the rarest DSD called ovotestes (found mainly in female 46 XX or 46XX/46XY mosaics/chimeras) despite the presence of both ovarian and testicular tissues, often within the same gonad, the reproductive organs are typically ambiguous and malformed and the rare subset of patients who are fertile are so as either males or females, not as both sexes. Here’s to give you an idea of the complexity of such a scenario, in 46 XX DSD patient.
And even in the case of the rarest DSD called ovotestes (found mainly in female 46 XX or 46XX/46XY mosaics/chimeras) despite the presence of both ovarian and testicular tissues, often within the same gonad, the reproductive organs are typically ambiguous and malformed and the rare subset of patients who are fertile are so as either males or females, not as both sexes. Here’s to give you an idea of the complexity of such a scenario, in 46 XX DSD patient.
The key to understanding this is that while people with atypical sex development are frequently infertile, when they are fertile, they are so as their biological sex. The presence of the opposite sex reproductive structures are never functional, because male and female are not interchangeable. This is why males with Kleinfelter’s, PMDS and AIS can father children (usually with help of assisted reproduction techniques), while females with XX testicular disorder cannot.
This is by no means an exhaustive list of DSDs, but I hope it is enough to explain the pattern. Yes some genes and sex differentiation processes might get mixed up, but it is the existing template of male (has Y) versus female (has no Y) that determines the outcome. For sex to be a “spectrum”, we would be seeing people right down the middle, who can self-fertilise because they are equal amounts male and female. There are no such cases recorded in medicine. If there was more than two sexes, we would be seeing people reproduce as something other than male or female. There are no such cases recorded in medicine either. There are only two gametes, sperm (male) and egg (female), male impregnates, female gets pregnant and gives birth to the young and very rarely the incredibly elegant yet complex process of sex differentiation goes wrong.
Unfortunately, in matters of sex, gender and women’s sport, science seems to be playing second fiddle to the Platonic ideal of what male and female are supposed to look/behave/think like, and we are witnessing idealised images of GI Joe and Barbie taking primacy over biological facts and unduly influencing the discourse.
Just a quick note about terminology. All disorders are differences, but not all differences are disorders. For example, being male versus female is a fundamental biological difference between two sex-classes of humans. But because they are there by design, so that our species can reproduce, these differences aren’t disorders. On the other hand, DSDs are disorders because they result in developmental anomalies which interfere with normal reproductive functions.
In a justified desire to remove stigma attached to illness and disability, patients, social justice activists and doctors have all been trying to move away from the pathologising language. Unfortunately, when we fail to use accurate language to describe things, other problems follow. Overzealous denial of pathology may lead to people being denied access to medical care, or it can lead to healthy people being unnecessarily medicalised. Such as in the case of gender clinics, where normally developed females who self-identify as male are diagnosed with a “testicular disorder”(a term that only reasonably applies to males whose testicles were removed, not developed or not functioning properly) and are given “testosterone supplementation”, while normally developed males who self-identify as female are diagnosed with “absolute womb factor infertility”(terminology that only reasonably applies to females whose uteruses didn’t develop normally or were removed) and are scouted for arguably impossible and illegal “uterine transplants”.
And in case of sport, male athletes are compelled by sporting authorities to medicate their natural physiology by means of testosterone suppression, in order to fit in a category to which they do not belong.
As far as I can tell, the rationale for allowing 46 XY male DSD athletes to compete with females has always been two fold – unfavourable comparison with the Platonic ideal of a man, and empathy. While unique physiology of male DSD athletes confers significant sporting advantage over female athletes, it usually doesn’t measure up to full male athletic performance. But beyond this cold, clinical fact, we can try to imagine what it must be like to be raised, train and believe you are female, perhaps even an athletics champion, only to find out that you are in fact biologically male. Not only does this cast a shadow on your sporting achievements, it changes how you think about yourself and your future. As females we expect to become mothers. We are treated a certain way by society. The way society conceptualises sexuality is based on whether we are attracted to the opposite sex, our own sex, or both. The implications of a late DSD diagnosis are huge, and come at tremendous personal cost.
This is perhaps why children with DSDs have been a target of much unethical experimentation in the past, including attempts to medically alter them in order to help them fit into the Platonic ideal of male or female. This might have been a noble intention initially, our society has low tolerance for people who are perceived as different, but unfortunately this rarely worked out for the best. If you research John Money, the man who both coined the phrase “gender identity” and developed the practice of gender reassigning intersex children and transgender adults, you will find terrible outcomes. And even though medicine has advanced a lot since, there is enduring evidence that “assigning sex” to DSD children doesn’t really work. A recent study of a large cohort of patients with 5ARD, a 46 XY male DSD I will talk more about in a minute, showed that all patients developed male gender identity, and those who were raised as girls went on to develop gender dysphoria and seek gender reassignment in keeping with their biological sex.
This is, consequently, the only area in which the phrase “gender identity” makes any sense, when it is applied to people with DSDs who have had their biological sex either incorrectly identified at birth, or “reassigned” as per above. And even when allowed to develop without medical intervention, due to bodily changes nobody without a DSD can fully comprehend, their gender identity might fluctuate and change. But this is in response to the body which they are trying to understand as they mature, not a purely psychosocial condition where a normally sexed male or female wishes or believes they are the opposite sex.
The incidence of DSDs, although overrepresented in female sport, is very small in the general population, about 0.018%. Transgenderism on the other hand is a much more difficult phenomenon to quantify because it relies on self-declaration. Whether transgenderism (which practices masculinisation of females and feminisation of males by means of opposite sex hormones and various degrees of surgery) is in fact compatible with the ethics of sport (which is supposed to be about what our natural bodies can do, not what drugs and surgery can do to our bodies) is a matter for another discussion. But judging by the ease with which these males have started to dominate female competition since their inclusion in the female category, it would be naive to assume they won’t come to be hugely overrepresented in female competitions as well.
The most prominent case in recent years that’s attempted to grapple with these incredibly complex issues is the case of Caster Semenya, a 46 XY DSD athlete who came to dominate female athletics competition due to male sporting advantage. In line with the current rules, Semenya was required to suppress her testosterone in order to compete in the female category. When she did, her sporting advantage declined accordingly. She fought for her right to not suppress her testosterone and lost. The question many are asking is whether this was the right decision. I think it was, only in a sense that it confirmed the importance of male sporting advantage. But I don’t think this decision is enough to safeguard female sport, and here is why.
Semenya was born with 5ARD, a DSD that only affects 46 XY biological males. An X-linked genetic mutation, 5ARD prevents the body from producing enough of steroid 5-alpha reductase 2, an enzyme responsible for converting testosterone into DHT, which is in turn responsible for development of male genitalia before birth. So babies with 5ARD are born with ambiguous genitals, micropenis, hypospadias or even female-appearing genitals. They can sometimes be mistaken for girls, or deliberately raised as girls, but if they are allowed to develop normally, and their testicles aren’t removed in a “gender assigning” procedure, they will experience male puberty, and with it, all the associated changed that will give them sporting advantage over female competitors,

5ARD isn’t the only male DSD that is relevant to this discussion, either. I recommend reading the article Natural Selection for Genetic Variants in Sport: The Role of Y Chromosome Genes in Elite Female Athletes With 46 XY DSD in which, despite muddled conclusions and continuous mis-sexing of 46 XY DSD athletes, the authors discuss the fact that rather than testosterone alone, it is the genes on the Y chromosome that are truly responsible for male competitive advantage.


 Reading this evidence only confirms that both female and male athletes are negatively impacted by the current rules – females by denying them fair play and males by forcing them to take testosterone-lowering drugs which don’t completely mitigate male sporting advantage but come with serious and long-term side effects. It is therefore astonishing that instead of making a case for the third category that could be designed to accommodate both DSD and transgender athletes, the authors argue that Y chromosome is “an example of an acceptable variable that contributes to athletic success in elite female athletes including those with 46,XY DSD”. In other words, in sport, males are the best females and the recent inclusion of trans-identified males (transwomen) in women’s sport is a result of sporting authorities following this logic to its natural conclusion. If female is nothing more than a low-testosterone male and she happens to have Y chromosome then good for her (and her team and country) as this is an “acceptable genetic variation”.
Reading this evidence only confirms that both female and male athletes are negatively impacted by the current rules – females by denying them fair play and males by forcing them to take testosterone-lowering drugs which don’t completely mitigate male sporting advantage but come with serious and long-term side effects. It is therefore astonishing that instead of making a case for the third category that could be designed to accommodate both DSD and transgender athletes, the authors argue that Y chromosome is “an example of an acceptable variable that contributes to athletic success in elite female athletes including those with 46,XY DSD”. In other words, in sport, males are the best females and the recent inclusion of trans-identified males (transwomen) in women’s sport is a result of sporting authorities following this logic to its natural conclusion. If female is nothing more than a low-testosterone male and she happens to have Y chromosome then good for her (and her team and country) as this is an “acceptable genetic variation”.
To say that a male is a genetic variation on a female is not a new assertion. But this variation goes back billions of years, and without it, there would be no humans in the first place. Furthermore, in humans, males and females are sexually dimorphic which means males are generally bigger, faster and stronger. So I reject the lazy attitude whereby anyone who doesn’t measure up to our idea of a male is automatically placed in a “non-male” ie. female category.
With regards to women’s sport, women have fought long and hard against prejudice and discrimination borne from their competitive disadvantage in relation to males. Also, women and girl athletes have been ogled, infantilised, underfunded, sabotaged and sexually assaulted because of their female sex, by those of male sex. And despite the enduring fight for rights of biological females to not be discriminated and dominated by males, they have had to cope with a sporting system that disadvantages them by including biological males.
I would like to reiterate that XY DSD athletes are not the same as trans-identified male athletes. They are different biologically and face very different challenges. However, for the purposes of inclusion in female sport, the two are related in practice, if not in spirit, and ultimately female athletes pay the price.
Women and girls are half the population and they deserve to compete fairly. Female athletes also have hopes and dreams of standing on the podium, proving their worth, getting sponsorships, or scholarships, prize money and a career in sport. Their self-esteem, sense of self and future prospects are all affected by the way current rules prioritise sporting advantage of biological males. I am here to ask that women’s human right of having access to single-sex spaces, which by definition includes female-only sport, is respected. Without exception.

Excellent very clear article, thank you. Beautifully argued. By the way here’s a link to that illuminating paper by Georgi K Marinov which you linked to. This one, in contrast, can be printed, copied &c https://www.nas.org/academic-questions/33/2/in-humans-sex-is-binary-and-immutable
LikeLiked by 2 people
Thank you Brian, I really appreciate it! I have also updated the link 👍
LikeLiked by 1 person
Absolutely excellent outline of the complexities; it is astonishing that so few medical authorities will stand up for women in this onslaught on their rights and very identity. Please circulate this to medical authorities with a request that they take a stand based on biology rather than societal pressure.
LikeLiked by 3 people
Could you write more about this: “A recent study of a large cohort of patients with 5ARD, a 46 XY male DSD I will talk more about in a minute, showed that all patients developed male gender identity, and those who were raised as girls went on to develop gender dysphoria and seek gender reassignment in keeping with their biological sex.”
What do you think is the reason? Is that the case with other DSDs as well? Can that be used as an argument that there’s a biological basis of gender identity?
LikeLiked by 1 person
Hi Anja! I think in this context, the phrase “gender identity” simply describes one’s understanding and acceptance of their biological sex. So what they’re saying here is only the people who were raised as the opposite sex developed a degree of distress (understandable, biologically based) and a need to announce their biological sex to the world (ie. gender transition). In their case this doesn’t require opposite sex hormones or body modification. Gender dysphoria in this context means dissatisfaction at being raised as the opposite sex. It is simply irrational to believe one is, or can become, the opposite sex. So the two contexts have been conflated. In DSDs I notice that phenotype plays a strong role, so women with CAIS or Swyer, even though biologically male, rightfully believe themselves to be women because phenotype apparently female, so much so that without modern medicine they would never know why they are infertile. But that is unique to DSDs. No degree of transgender transition can so fundamentally mismatch your genotype and phenotype as DSDs do. Plus, in DSDs the process is entirely natural and spontaneous. This is such a complex area of medical care, it requires multidisciplinary team approach and being patient-led in terms of which biological sex they feel most comfortable with presenting socially. This however doesn’t mean true biological sex can be disregarded in situations where sex does matter, such as in medical care and sport. The more matched genotype to phenotype is, or becomes, such as in the case of 5ARD, the more sex and gender identity will match. What happens in case of trans people is completely different. They describe feeling distressed, but the distress comes from wanting to modify a healthy body. This resembles body dysmorphia, and the distress seldom goes away even after transition, because the explanation the mind came up to explain dysphoria was wrong in the first place. Gender ideology misapplied the DSD-specific concepts and language to a very different patient population. But ultimately this was unhelpful to both trans people and people with DSDs. Research that should be going into DSDs is not happening and trans people aren’t given the psychological help they need. The affirmative model and “Memorandum of understanding” misrepresents the actual help trans people need as “conversion therapy” and the treatments they do offer only solidify the performance of gender. Thanks again for your question, it really made me think. 👍
LikeLiked by 2 people