Authors: Dr S. Helyar, A. Hill and Dr L. Griffin
Background
Stonewall is the UK’s leading LGBT charity. It began as a lobbying organisation in 1989 and incorporated transgender rights into its formal remit in 2015. A key, and highly successful strategy has been the introduction of the Stonewall Diversity Championship Scheme. Organisations pay Stonewall for training and guidance to facilitate the adoption of a specific agenda which promotes trans- inclusivity through the implementation of policies to be embedded within organisational culture. These include trans specific guidance and toolkits. Stonewall champions are then offered the opportunity to earn a place on its Workplace Equality Index, in which scheme members are evaluated and ranked according to how well their policies and procedures align with Stonewall’s principles. The top 100 organisations are then ‘publically celebrated’.
Our Concerns with nursing’s affiliation and association with the Stonewall Diversity Championship Scheme
The history of Stonewall to promote equality and safeguard the rights of the LGBT community is one to celebrate. However nursing affiliations should be based on recognition of the evidence base, not ideology and judged on current record and strategy, not legacy achievements and reputation.
There are a number of publicised potential risks associated with becoming a Stonewall champion, particularly for public and professional bodies. These risks have been itemised in this comprehensive critique of Stonewall’s strategy drafted by a feminist legal team here.
Importantly, we believe that as a profession, there is specific risk to the reputation of nurses and our ability to work within our code of conduct from continued affiliation with Stonewall. We are concerned that Stonewall has spoken out against the recent Tavistock V’s Bell ruling which many view as a victory for child safeguarding against the experimental medicalisation of gender dysphoric children. We object to the undue influence that Stonewall, an unelected body, has been allowed to exert on healthcare providers to shape policy which does not align with the law and includes aspects likely to force nurses to practise against our code. We outline our concerns as nurses who love and care deeply about our profession and patients. The nursing profession stands distinct as the most trusted, governed by our code which demands high standards of practice and behaviour including; integrity, safeguarding, evidence based practice and a professional obligation to raise concerns and prevent reputational damage. We call on healthcare professional organisations, trade unions, the nursing professoriate and the nursing regulator to withdraw from the Stonewall’s Diversity Championship Scheme and for senior nurse practitioners, academics and other nurse leaders to also advocate for removal.
Summary of key objections:
1. Medical care of children and young people
The judicial review arising from Bell v Tavistock raised concerns about the medical interventions offered to children and young people with gender dysphoria. Evidence of benefit has not been established and the potential for harm was determined to be substantial. Effects of puberty blockers followed by cross sex hormones include reduction in bone density, loss of sexual function and sterility. Moreover, there are unknown effects on brain development (NICE 2021). The role of puberty blockers in initiating full medical transition was also highlighted in the ruling as 98% of children prescribed blockers went on to cross sex hormones. It was ruled that children, depending on their age, are either unable or are unlikely to be able to provide informed consent for such experimental interventions. Since this ruling, Sweden suspended these treatments for the under 18s and proposed to only prescribe them in context of carefully designed and monitored randomised control trials.
This ruling appears to be very much in keeping with our code e.g. providing evidence based treatment, safeguarding children and integrity. Stonewall has objected to the ruling. We have the following concerns regarding Stonewall’s published response. The subsequent Appeal related primarily to Court jurisdiction and does not counter these concerns.
• Stonewall continues to demand medical interventions for children based on the affirmation model.
• Stonewall maintains that puberty blockers are reversible, which conflicts with NHS guidance that the long term effects are unknown.
• Stonewall states that children can provide informed consent for puberty blockers. The inference is therefore that children as young as 13 years of age can consent to sterility and loss of sexual function in adulthood.
• Stonewall fails to acknowledge the 61-98% of children who, without medical intervention, desist. That is, naturally stop opposite sex identification. Similarly, it fails to acknowledge the 25-fold rise in referrals to the Tavistock Gender Identity Development Service since 2009. These are disproportionately girls, many of whom will grow up to be same sex attracted, or children with co-morbidities or traumas who are seeking medical intervention. A failure to be both intellectually and clinically curious about these findings is at odds with effective advocacy for gender non-conforming youth.
• Stonewall claims that denying children who present with gender dysphoria puberty blockers, is ‘not a neutral act’, thereby pathologising puberty, a natural and necessary process for human development.
• Stonewall asserts that the most common reason for detransition is lack of family and community support, and that regret is usually due to dissatisfaction with a surgical procedure. It ignores the growing numbers of detransitioners, such as Keira Bell, the claimant in the judicial review, whose case rested on her claim that the affirmation model, promoted by Stonewall, actively harmed her. Stonewall has remained silent on the subject of healthcare provision for detransitioners despite this group having very specific clinical needs.
We believe this is the medical scandal of our age and continued affiliation with Stonewall implies nurses’ support for Stonewall’s position against the evidence base, potentially against the law and against our commitment as nurses to support child health, welfare and development. As such, we believe this will bring the nursing profession into disrepute. Recent reviews by the National Institute for Health and Care Excellence on the clinical effectiveness, safety and cost-effectiveness of puberty blockers and cross sex hormones concluded that the evidence base of impact on gender dysphoria, mental health and quality of life is of low, or very low quality. At best, we would urge all nursing bodies to formally adopt a neutral position regarding the transitioning of children and young people.
2. Misrepresentation of equality law
There are a number of protected characteristics under the Equality Act (2010) including sex, age, sexual orientation and gender reassignment. It must be understood that no one characteristic trumps any other. People cannot be discriminated against because of gender reassignment (e.g. you cannot deny someone a standard job because they have had gender reassignment) but that does not mean single- sex provision cannot exclude anyone who isn’t female. Under the Equality Act (2010), when there is a conflict between the needs of various groups with protected characteristics, it is still permissible to discriminate on the grounds of sex, if it is a proportionate means to achieve a legitimate aim. A hospital ward, where patients are, by definition, vulnerable and dependent on the environment for safety, privacy and dignity (e.g. unwell, sleeping, in various states of undress, receiving intimate personal care by the bedside, confused, etc) would appear prima facie to meet the definition of proportionality.
Stonewall campaigns for the removal of the Equality Act (2010) single-sex exemptions, and as such, places it in direct conflict with a core national NHS same-sex accommodation policy with the strategic aim to ensure safety, privacy and dignity for patients. Stonewall misrepresents equality law and single- sex spaces in its guidance to championship scheme members and measures placement of scheme members on its Workplace Equality Index based on this guidance.
• The Equality Act (2010) makes provision for single-sex services. Organisations can provide services that are separate, different and/or be provided to only one sex. However, Stonewall’s guidance, whilst acknowledging that there are some circumstances where trans people who are male can be legally excluded, states that any such exclusion requires a ‘high barrier of proof’. This concept of ‘a high barrier of proof’ does not exist in law. Instead, the law cites clear, readily defined and highly achievable examples of where single-sex provision is considered proportionate, e.g. changing rooms, hospital wards, domestic violence shelters, and when a person might reasonably object if another user is of the opposite sex. Therefore, Stonewall falsely informs championship scheme members that single- sex provision cannot, in all probability, be lawfully implemented. This is simply not true.
• Stonewall informs organisations that individuals have the right to access single-sex facilities based on gender identity, and that refusal on this basis is illegal. The term ‘gender identity’ is not a protected characteristic nor a term recognised in law. Exclusion on this basis cannot therefore be a breach of the law. Stonewall is thus providing false information to championship scheme members about the basis on which an individual can access single-sex spaces and whether or not they can be lawfully excluded. This is causing immense confusion in numerous contexts where single-sex exemptions are invoked. For example, the Oxfordshire Council Trans Inclusion Toolkit for schools had to be withdrawn after an Oxfordshire schoolgirl took the Council, a Stonewall Champion, to the High Court because of its misrepresentation of equality law. This is mirrored by Warwickshire County Council whose guidance as advised by Stonewall also had to be withdrawn.
• Stonewall has been a key player in leading the campaign for reform of the Gender Recognition Act (2004). Proponents of reform are arguing that the current legal process by which sex markers can be legally changed on official records is relaxed and is replaced by a process of self-identification, or ‘Self-ID’. This would enable a person to change their legal sex by a simple statutory declaration, rather than the current process that involves a legal process including a medical assessment. Should self-ID become law, there would no longer be any mechanism to prevent men accessing female spaces, as all they would have to do is claim to identify as women. As yet, self-ID is not lawful. Proposals to introduce self-ID were rejected by Government following strong campaigning by women’s groups. Despite this, Stonewall advise that access to single-sex provision is based on self-ID. Therefore, Stonewall provides false information on the legal mechanisms in which an individual can access single-sex spaces.
These misrepresentations are of concern because a number of organisations tasked with commissioning or delivering health, as well as clinical regulatory and educational bodies have used Stonewall guidance to inform local policies, usually as a core part of sign up to membership of the Stonewall Diversity Championship Scheme. This has led to the development of a culture in which misapplication of equality law is commonplace, particularly to the detriment of women and girls.
3. The treatment of women in healthcare settings and application of the Equality Act (2010)
Through the active campaigning by Stonewall to remove single-sex exemptions and its advocacy for access to single-sex spaces to be based on gender identity rather than sex, the role of nurses to advocate and safeguard for some of our most vulnerable female patients is compromised.
In hospital settings, where patients are by definition, vulnerable, they have a right in law, the NHS Pledge and the CQC regulations to be accommodated in single-sex spaces. Where there is no meaningful definition of ‘transgender’, Stonewall’s umbrella definition being over-inclusive and vague, how can one determine who is ‘truly trans’ and who might want access to vulnerable patients for other reasons?
Where female patients are nursed in bed, often in states of semi-undress, unable to defend themselves due to illness, confusion or frailty, and require intimate care at the bedside, nurses and the environment are entirely depended upon to uphold and maintain their safety, privacy and dignity.
In mental health settings, women are particularly vulnerable. They are often held under the Mental Health Act, and are therefore unable to leave, even when they are placed in dangerous situations. These patients often struggle to self-advocate, and rely on staff to uphold safeguarding. Importantly, when under section, these women do not have recourse to the police and judicial system should an unwitnessed sexual assault occur because they lack capacity. There is a high rate of sexual trauma amongst women who become users of mental health services and there was a 2018 CQC report that highlights the danger of sexual violence against in-patients in mental health settings. These women are therefore disproportionately dependent upon single-sex hospital provision for safety and therapeutic care.
Where conflict between the needs of two or more groups with protected characteristics arises, it is necessary to carry out Equality Impact Assessments. Impact assessments provide the opportunity for organisations including hospital trusts to ensure policies balance fairly the rights of all patients in line with equality legislation. The desires of one group cannot be allowed to trump the safety, privacy and dignity of any other. The purpose and process of carrying out such an assessment is outlined here and involves a meaningful process of engagement and involvement with all the relevant stakeholder groups in order to ascertain whether the implementation of anti-discrimination policies risk impacting on groups with other protected characteristics.
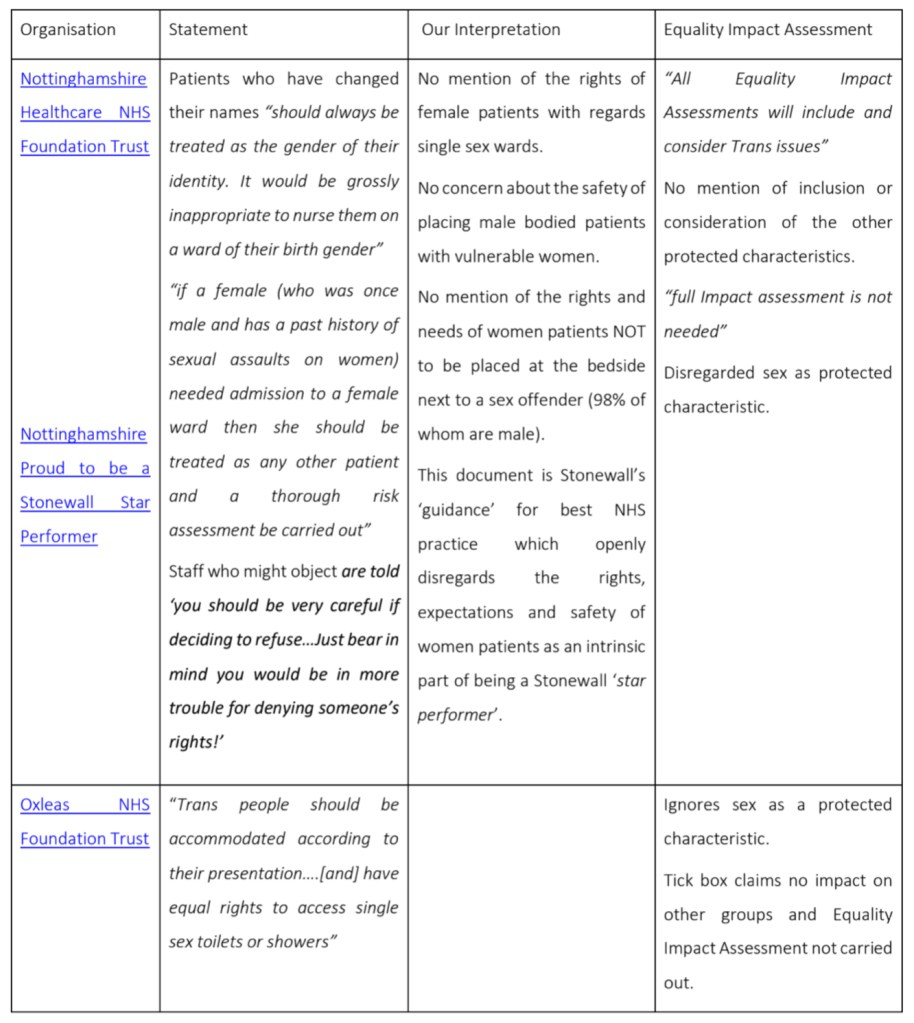
In reality, many Stonewall champions have implemented policies informed by guidance from Stonewall described above and have not carried out meaningful and robust impact assessments. A plethora of trans accommodation policies, mainly to be enacted by nurses, have been implemented by health organisations throughout the UK with little or no regard for the safety, privacy, and dignity of other patient groups, particularly women. Examples of Stonewall linked policies (as Champions or informed by) used in various NHS settings implemented with no consideration to the needs of other groups, and with aspects likely to go against our code of conduct include:
[NOTE: The table below doesn’t look the best on smartphone browsers, so below you can view the gallery with screenshots of the below table (without the working links), or alternatively please feel free to download the pdf of this document]
| Organisation | Statement | Our interpretation | Equality Impact Assessment |
|---|---|---|---|
| Nottinghamshire Healthcare NHS Foundation Trust Nottinghamshire Proud to be a Stonewall Star Performer | “Patients who have changed their names “should always be treated as the gender of their identity. It would be grossly inappropriate to nurse them on a ward of their birth gender” “if a female (who was once male and has a past history of sexual assaults on women) needed admission to a female ward then she should be treated as any other patient and a thorough risk assessment be carried out” Staff who might object are told ‘you should be very careful if deciding to refuse…Just bear in mind you would be in more trouble for denying someone’s rights!’ | No mention of the rights of female patients with regards single sex wards. No concern about the safety of placing male bodied patients with vulnerable women. No mention of the rights and needs of women patients NOT to be placed at the bedside next to a sex offender (98% of whom are male). This document is Stonewall’s ‘guidance’ for best NHS practice which openly disregards the rights, expectations and safety of women patients as an intrinsic part of being a Stonewall ‘star performer’. | “All Equality Impact Assessments will include and consider Trans issues” No mention of inclusion or consideration of the other protected characteristics. “full Impact assessment is not needed” Disregarded sex as protected characteristic. |
| Oxleas NHS Foundation Trust | “Trans people should be accommodated according to their presentation….[and] have equal rights to access single sex toilets or showers” | Ignores sex as a protected characteristic. Tick box claims no impact on other groups and Equality Impact Assessment not carried out | |
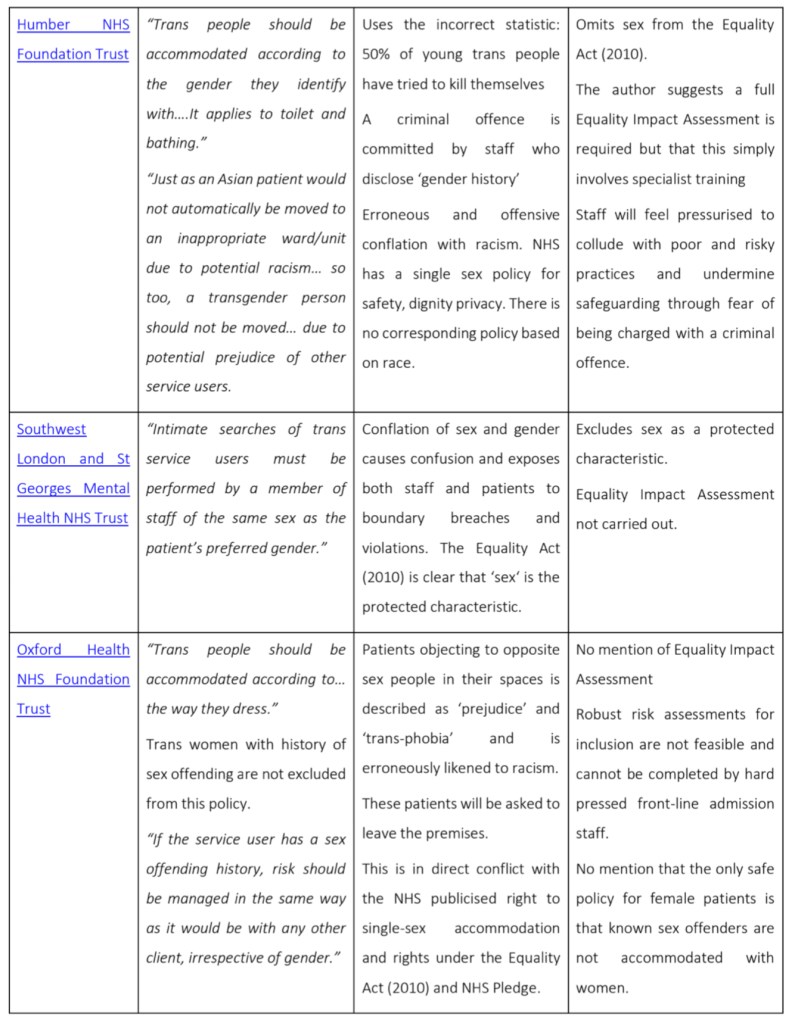
| Humber NHS Foundation Trust | “Trans people should be accommodated according to the gender they identify with….It applies to toilet and bathing.” “Just as an Asian patient would not automatically be moved to an inappropriate ward/unit due to potential racism… so too, a transgender person should not be moved… due to potential prejudice of other service users.” | Uses the incorrect statistic: 50% of young trans people have tried to kill themselves. A criminal offence is committed by staff who disclose ‘gender history’ Erroneous and offensive conflation with racism. NHS has a single sex policy for safety, dignity privacy. There is no corresponding policy based on race. | Omits sex from the Equality Act (2010). The author suggests a full Equality Impact Assessment is required but that this simply involves specialist training Staff will feel pressurised to collude with poor and risky practices and undermine safeguarding through fear of being charged with a criminal offence. |
| Southwest London and St Georges Mental Health NHS Trust | “Intimate searches of trans service users must be performed by a member of staff of the same sex as the patient’s preferred gender.” | Conflation of sex and gender causes confusion and exposes both staff and patients to boundary breaches and violations. The Equality Act (2010) is clear that ‘sex‘ is the protected characteristic. | Excludes sex as a protected characteristic. Equality Impact Assessment not carried out. |
| Oxford Health NHS Foundation Trust | “Trans people should be accommodated according to… the way they dress.” Trans women with history of sex offending are not excluded from this policy.” “If the service user has a sex offending history, risk should be managed in the same way as it would be with any other client, irrespective of gender.“ | Patients objecting to opposite sex people in their spaces is described as ‘prejudice’ and ‘trans-phobia’ and is erroneously likened to racism. These patients will be asked to leave the premises. This is in direct conflict with the NHS publicised right to single-sex accommodation and rights under the Equality Act (2010) and NHS Pledge. Staff told that disclosing trans status is a criminal offence and that the staff might result in a prison sentence. | No mention of Equality Impact Assessment Robust risk assessments for inclusion are not feasible and cannot be completed by hard pressed front-line admission staff. No mention that the only safe policy for female patients is that known sex offenders are not accommodated with women. |
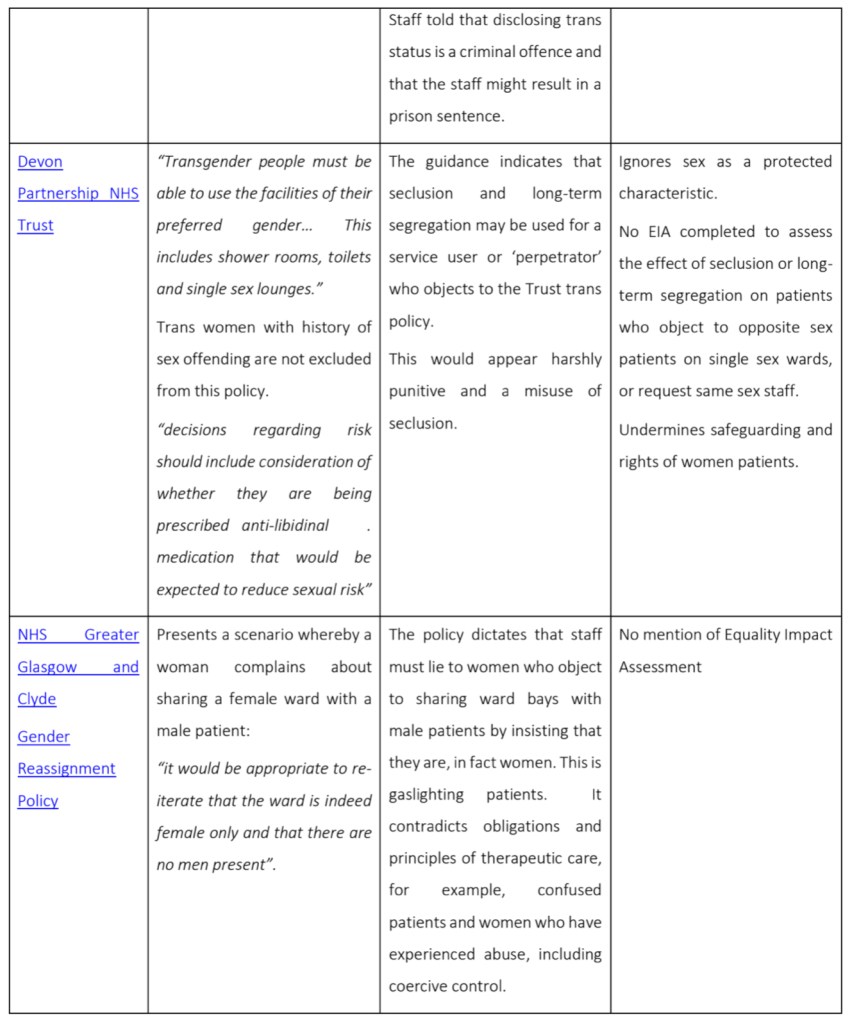
| Devon Partnership NHS Trust | “Transgender people must be able to use the facilities of their preferred gender… This includes shower rooms, toilets and single sex lounges.” Trans women with history of sex offending are not excluded from this policy.” “decisions regarding risk should include consideration of whether they are being prescribed anti-libidinal . medication that would be expected to reduce sexual risk” | The guidance indicates that seclusion and long-term segregation may be used for a service user or ‘perpetrator’ who objects to the Trust trans policy. This would appear harshly punitive and a misuse of seclusion. | Ignores sex as a protected characteristic. No EIA completed to assess the effect of seclusion or long- term segregation on patients who object to opposite sex patients on single sex wards, or request same sex staff. Undermines safeguarding and rights of women patients. |
| NHS Greater Glasgow and Clyde Gender Reassignment Policy | Presents a scenario whereby a woman complains about sharing a female ward with a male patient: “it would be appropriate to re- iterate that the ward is indeed female only and that there are no men present”. | The policy dictates that staff must lie to women who object to sharing ward bays with male patients by insisting that they are, in fact women. This is gaslighting patients. It contradicts obligations and principles of therapeutic care, for example, confused patients and women who have experienced abuse, including coercive control. | No mention of Equality Impact Assessment |
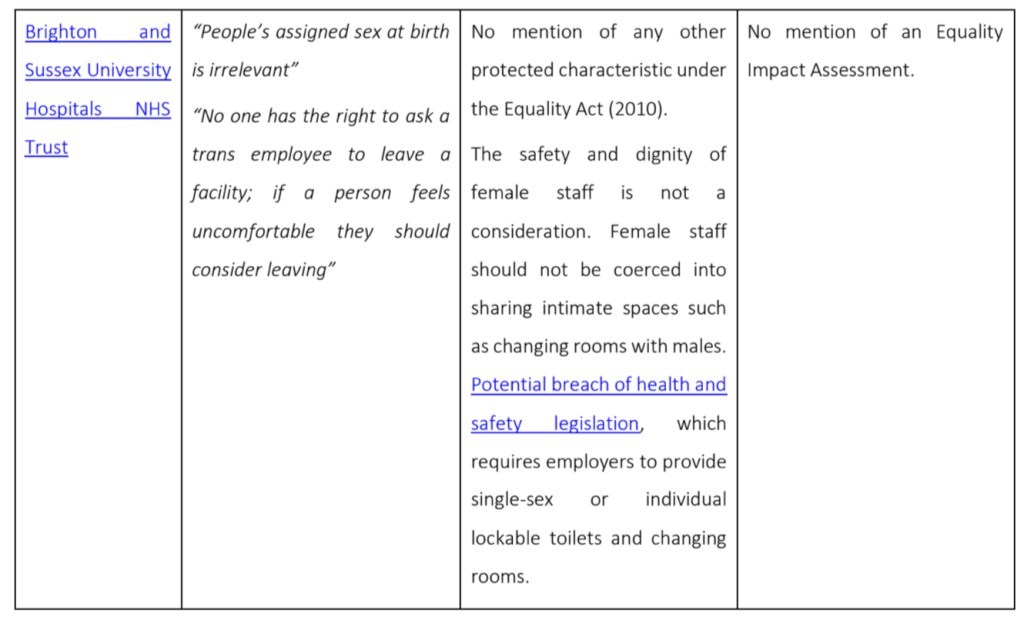
| Brighton and Sussex University Hospitals NHS Trust | “People’s assigned sex at birth is irrelevant” “No one has the right to ask a trans employee to leave a facility; if a person feels uncomfortable they should consider leaving” | No mention of any other protected characteristic under the Equality Act (2010). The safety and dignity of female staff is not a consideration. Female staff should not be coerced into sharing intimate spaces such as changing rooms with males. Potential breach of health and safety legislation, which requires employers to provide single-sex or individual lockable toilets and changing rooms. | No mention of an Equality Impact Assessment. |
Failure to understand the purpose and function of Equality Impact Assessments has led to many providers losing sight of their responsibility to protect the rights of all patients, and resulted in a failure to meet their Public Sector Equality Duty. The underlying approach of all these policies is to punitively disregard the needs and rights of women patients for single-sex provision.
The difficulties in balancing the conflicting rights of the various groups under the Equality Act (2010) has been illustrated by the Equality Impact Assessment carried out retrospectively by Bristol, North Somerset and South Gloucestershire CCG (BNSSG). This commissioning group, then a Stonewall champion, attempted a post-hoc EIA for their toolkit ‘Supporting Trans People: Best practice guidance for health and care practitioners’, after multiple complaints about its contents from clinicians, patients and women’s groups. In common with other such trans-inclusion policies, the toolkit explicitly prioritises the needs of trans patients when considering which ward to admit to. A robust impact assessment was then conducted, which included meetings with various stakeholders including a group of local clinicians, a women’s group and members of the public. The impact assessment was published and clearly demonstrates the difficulty in resolving the conflicting needs of the various groups. The BNSSG withdrew its guidance and has withdrawn from Stonewall’s Diversity Championship Scheme.
Importantly, many policies undermine safeguarding. Healthcare providers and other organisations are eagerly signing up to the Championship Scheme and working hard to embed trans policies into their organisational structures. There is a risk that questioning any aspect of these policies will be perceived as ‘anti-trans’. Organisations are actively primed to avoid anything that might suggest transphobia even when there are serious safeguarding concerns. Staff are less likely to report legitimate concerns, as professionally obliged, fearful of discipline or censure. This is exemplified where Stonewall advises as NHS ‘best practice’ (above in table – Nottinghamshire) that male sex offenders – with a history of sex offending against women – who identity as women should be admitted to a female ward, ‘subject to a risk assessment’. Nurses are also informed that they must ‘careful’ if refusing admission, that they may find themselves in ‘more trouble’. Stonewall guidance denies the professional autonomy of nurses to make decisions to take account of the needs of all our patients, even in a clear safeguarding situation, and implicitly threatens and bullies nurses. Another example is Sonia Appleby, the Safeguarding Lead at the Tavistock and Portman Trust who claims she was targeted for raising patient safeguarding concerns. We believe that Stonewall policies run the risk of allowing harm to be caused to certain groups and it would be difficult to defend these policies should a legal challenge or complaint arise either against organisations or individual nursing staff enacting these policies.
4. The safety of other vulnerable groups
• We have seen evidence that Stonewall has cherry picked the evidence on women’s refuges, which undermines trauma-informed patient centred therapeutic services for women escaping violence.
• Stonewall worked alongside other organisations so that access to the women’s prison estate in Scotland is based on self-ID and not sex.
• In England and Wales, the Ministry of Justice (MoJ), a Stonewall Champion, implemented Stonewall policy and allowed the placement of males into women’s prisons based on gender identity. The MoJ was sued by a female prisoner who alleges she was sexually assaulted by a male inmate whilst in prison. The Judge acknowledged the conflict of rights and risk to women prisoners if males were accommodated with them; that women would experience ’fear and acute anxiety‘ from sharing with a male, particularly if the male has been convicted of a sexual crime; the increased risk of harm to women; and that the public would think it “incongruous and inappropriate that a prisoner of masculine physique and with male genitalia should be accommodated in a female prison in any circumstances“. Whilst the judge ruled that the policy could be operated lawfully, (not withstanding that it is equally lawful to exclude all male prisoners), it can only do so if significant risk mitigation procedures are implemented for the safety of women, in contrast to Stonewall’s open door policy, based on gender identity.
• These prison policies advocated by Stonewall ignore the right of women to single-sex provision, the vulnerability of women prisoners who have already experienced high rate of sexual trauma and the actual risk that these policies introduce to them. Where trans prison policies have been implemented without regard to the safety of women, abuses have occurred. One example is Karen White, a convicted sex offender, who was convicted of sexually assaulting two female prisoners whilst in the women’s estate. It is deeply concerning for nursing bodies to be affiliated with a body which seemingly gives so little regard to the safety and dignity of these women.
• Incarcerated women have an absolute right to be protected by responsible authorities from rape. Should a woman be raped or made pregnant whilst in prison or detained under the Mental Health Act, something has gone horribly wrong. The Nursing profession must in its advocacy, affiliations and policy safeguard these women with a definitive position that any risk allowed in policy of rape or pregnancy to them whilst in the care of the NHS or prison service is unacceptable, and that the only acceptable policy is one of zero risk.
Adult, mental health, domestic violence specialist and prison nurses have a duty of care and responsibility to advocate, safeguard and provide patient centred care for our highly vulnerable and dependent women patients. We believe that nursing affiliation with Stonewall, whose position and campaigning would lead to increased risk of assault, introduce actual risk of pregnancy and rape to female inmates and patients, and undermine provision for women escaping violence, compromises this duty.
5. Behaviour towards those who speak out on the subject of gender ideology or challenge Stonewall’s influence.
• Stonewall is being sued by Allison Bailey, a black lesbian barrister, survivor of childhood sexual abuse and co-founder of the charity LGB Alliance. Bailey alleges that Stonewall pressurised her chambers, a Stonewall Champion, to sanction her, for defending the rights of women and lesbians, and through associations with Women’s Place UK and LGB Alliance.
• In their communication to Bailey’s chambers, Stonewall implied that Women’s Place UK, a women’s rights group which actively campaigns to uphold the Equality Act (2010), and has presented formal submissions to a Parliamentary Select Committee, were a ‘hate group’. We would argue this accusation is totally unfounded.
• Taken together, Stonewall’s mantra of ‘no debate’, its labelling of women’s rights groups as ‘hateful’ and its bullying of those individuals who speak out, results in a chilling effect of freedom of speech and association. These behaviours are disproportionally targeted at women and risk having a detrimental effect on women’s lives and rights. We are especially concerned about women whose employer, university, union, and/or regulatory body are Stonewall Diversity Scheme Champions, and fear that any discussion of women’s sex based rights, including the rights and needs of female patients, as professionally required, risk being compromised.
Most nurses are women and therefore this will have a disproportionate effect on nurses whose rights to freedom of speech, political association and ability to advocate for all patients, including our women patients, must be upheld.
6. Use of inaccurate terminology and reframing of language.
There is increasing pressure from Stonewall for healthcare organisations to adopt language that is based on ideology and not scientific fact, in order to prevent the word ‘woman’ to be linked to female biology.
• Stonewall defines sex as being ‘assigned at birth’. This is scientifically incorrect and misleading. Sex is determined at the point of fertilisation and revealed at, or often before, birth. Nurses have a duty to ensure healthcare language is accurate, clear and retains public confidence. We see no reason why nurses should not use a definition which is both factually correct and sensitive to the needs of transgender people.
• This definition disregards and negates the needs of other patient groups where recognition and language that sex is determined at conception is vital to care and advocacy, e.g. management of sex- related syndromes in-utero. It also fails to recognise the international outrage of sex-selected abortion against unborn girls. Estimates suggest over 45 million unborn girls have been terminated over the last 50 years due to recognition that sex is determined pre-birth.
• Many people reject the notion of an inherent gender identity. Many people regard ‘cis-gender’ offensive, especially many women, as it suggests that they naturally identify with feminine stereotypes, which are ascribed a second class status.
• The use of ‘cis’ is not a neutral statement of fact that just means ‘not trans’, it actively ascribes a belief or identity onto another individual, when one may not exist or be rejected. Most of our patients are classed as ‘cis’ and will have no idea about this concept, and many nurses, the majority of whom are women, would reject this label.
• Stonewall encourages organisations, including healthcare trusts, to adopt the use of ‘gender neutral’ language in sex-relevant policies as part of being a Stonewall champion. These policies are then awarded points which go towards a ranking within the Workplace Equality Index. Examples of Stonewall approved language includes the removal of ‘mother’ and ‘father’ to be replaced with ‘pregnant employee’, ‘parent who has given birth’ or ‘second parent’.
• Many will deem the demands of Stonewall to remove the naming and language of pregnant women and new mothers and fathers offensive and exclusionary. In particular, it denies the profound and life-changing reality of pregnancy and motherhood for women and goes contrary to the role of nurses to provide person-centred and holistic care for all individuals and communities.
• The power and influence of Stonewall is such that many other organisations are adopting similarly gender neutral language. Many argue that words and phrases are being used that are both confusing and dehumanising to describe women and their bodies. This impacts on healthcare. Examples include the Scottish Government, which has removed the word woman in its cervical cancer screening healthcare campaign despite the fact that, for example, nearly half of women do not know what a cervix is and need these words to signpost to cervical screening, which for some, will be lifesaving.
• NHS Digital has an entire Pronouns Guide which includes the phrase: “Over time, this will help your brain rewire how it thinks about an individual’s pronouns”. We find it deeply concerning that Stonewall, not only thinks it has the remit to rewire our brains, but that it so confident, it is actually written into NHS policy.
Conclusion
Nursing bodies must have the highest regard in terms of its affiliations. We believe Stonewall’s recent activities no longer align with the values of nurses which require evidence based practice, support for child development, informed consent, safeguarding, accurate and fair implementation of equality legislation for the benefit of all patients, zero-tolerance to any form of bullying and an understanding that true inclusion requires language, including sexed-based language when relevant, that reflects the needs of all patients.
We ask nursing bodies, where relevant, to form a separate position on the treatment and care of children and young people who present with gender dysphoria from that of our adult patients, which reflects their distinct child development and healthcare needs, aetiology, co-morbidities/traumas and evidence base. This will help safeguard and ensure high standards of therapeutic care for all children and young people who present with gender dysphoria, and enable the many who would naturally desist, to do so, without medical intervention and long term harms.
We believe that all nursing bodies must support in terms of policy and affiliation, organisations who uphold equality law, for the safety, dignity and privacy of all our patients. In particular, we ask that nursing bodies be unequivocal in its position that the risk of pregnancy and rape to our incarcerated women patients in policy must be one of zero risk.
Due to the high regard and trust in which nurses are held by the public and our duty to uphold the highest standards of practice, we believe nursing bodies show the moral leadership that our patients expect and depend upon of us and withdraw, or lobby for the wider organisation to withdraw from the Stonewall Diversity Championship Scheme.

Thank you, thank you, thank you! So perfectly articulated!
LikeLiked by 4 people
Thank you so much for this statement—clear, incisive, comprehensive. I will do my best (not much, I realize) to alert friends and family to it.
LikeLiked by 3 people
Thank you. As a nurse myself I am deeply concerned about the issues you raise & I wholeheartedly support this statement.
LikeLiked by 3 people
This is a stunningly articulate, rational and ethical statement.
Denise
LikeLiked by 3 people
I am in tears. This is so important to me as a nurse. I have not felt able to share what I believe to be true and right with colleagues.
We are being silenced and stonewall (an organisation I once admired) is leading the mob silencing us.
Thank you
LikeLiked by 3 people
Thank you for your comment Dorothy. You are not alone, far from it! Please feel free to download the document (link at the top of the page) and share it with colleagues. Following Maya Forstater ruling, employers are no longer leglly permitted to discriminate or harass people who are concerned about impact gender identity policies.
LikeLiked by 1 person
Thank you so much!!
At last, a concerted & articulate rebuttal by nurses of these harmful, unhelpful, illegal & coercive Stonewall Guidelines.
LikeLiked by 2 people
This is an exceptional appraisal of the current position and its relationship with professional practice. Thank you so much for such a brave and thoughtful piece of work. Neale
LikeLiked by 2 people
Thanks so I much for summarising and putting forward the thoughts and experiences of many You’ve pointed to so many legitimate concerns about Stonewall’s coercive behaviour. Many in the LGB community and the T community are concerned about what’s going on and the consequences of it, particularly for women. Well said.
LikeLiked by 2 people
Thank you. This issue is so important and this letter is so clear as to why.
LikeLiked by 2 people
A very clear and systematic set of arguments that we can use in any policy discussions, whether as originators or recipients of services.
LikeLiked by 2 people
Very well-explained, reasonable, and important.
LikeLiked by 1 person
Thank you so much, thoughtful, clear and concise, many will find this invaluable
LikeLiked by 2 people
As a nurse I am so glad to see this. The Nursing & Midwifery Council’s response to the Scottish self-ID consultation was worrying.
LikeLiked by 3 people
Beautifully articulated and likely to be a go to reference for lots of people. Thank you for all that work. Superb!
LikeLiked by 2 people
As a mental health nurse (now retired from paid work) my impotence in the face of the relentless undermining of women’s sex-based rights, as nurses and as patients, has been a source of real distress to me. I salute those of you who have found the time and energy to organise this defence and thank you, from the bottom of my heart.
LikeLiked by 1 person
Thank you so much for this very clear and unambiguous discourse on your deeply held concerns and ambitions for the nursing and healthcare professions going forward. These concerns are shared right across these professions and as professions concerned with the safety of not only the patients in their charge, but the safety and integrity of the professions themselves, it is not only right that concerns are raised from within, but it would be morally and ethically repugnant for those concerns to remain silenced. Indeed as the whole ideological framework has shown over the past five years or so within the UK, it is the silencing and fear of professional retribution which has allowed the ‘advancement’ of this awful strategy towards who knows what horrific outcomes within our society as a whole. We cannot sit in silence, watchfully waiting to see what the next step or who the next victim will be. May your voices grow stronger and your concerns be amplified ASAP.
LikeLiked by 1 person
Thank you!
I have taken the difficult decision to refuse hospitalisation because of the risk of being placed in a ward along side men pretending to be women, or indeed having to endure intimate procedures or help with personal care by a man who insists he’s a woman.
I look forward to the day when hospitals once again respect the rights and safety of women.
LikeLiked by 1 person
Dear Sue, as a woman who lives with chronic illness, I am devastated that all of us are put in a situation to self-exclude from medical care because of these unconscionable, cruel and dangerous policies. I feel so sad and angry. I hope your health doesn’t suffer because of this. xx
LikeLike
The Trans Ideology is imposing compelled and inaccurate speech and thought. Norfolk and Norwich University Hospitals NHS Foundation Trust sent out a review of Outpatient Services, asking my Gender. They also do this for maternity services. I pointed out to them that Gender has no scientific validity, and since they were obviously not interested in accuracy, as a 58 year old women of White heritage, I had decided to identify for the purposes of their survey as a 15 year old girl of Afro Caribbean extraction. I have every sympathy for people who feel they are in the “Wrong Body”, but the scientific reality is it is not possible to change sex. That must be the starting point.
LikeLiked by 1 person
I have also been in the position of requiring Post Operative care. In spite of my request for same sex carers for intimate care, I was sent two blokes. If Stonewall has its way they would only have to announce they identified as women and rejecting them potentially could have been in the local police stations holding cells for hate crime.
LikeLiked by 1 person
With Ofcom and the BBC both recently pulling out of their membership and biased association with Stonewall, following the incredible investigation by Stephen Nolan (BBC sounds) others need to follow suite. I had no idea that my public body to who I pay money every year was also in with Stonewall. Horrified! #comeoutofstonewall
LikeLiked by 1 person
Has there been any response from the RCN or NMC about Stonewalls position or their position on sex and gender?
LikeLiked by 1 person
Eventually it will become known what’s been going on behind the scenes. All I can say is that, the more nurses join in, the quicker we will see the desired outcome. xx
LikeLike
You are free to identify as anything you want, but you can not expect others to share your beliefs. You were polite, which I am grateful for 👍
LikeLike