written by Anonymous
Yes, you read that correctly. A man who wishes to have breast surgery as part of his gender affirming care is now more eligible for funding to make his non medically necessary, dysphoria induced dreams come true over my, a natal woman’s, need to have a congenital issue resolved. All I can say is thank heavens that the NHS still accept breast cancer survivors and the recipients of dangerous implants as a priority – but you never know, soon this too may be recognised as a luxury cosmetic procedure!
This is all of our responsibility. In truth, I have very little recollection of how we got here. The attacks against my sex have been subtle – a Venus symbol carefully removed from my sanitary pads, a TED Talk introducing the word ‘womxn’, the lavatory in a London Pub with a ‘Ze’ plaque (whereby a man accidentally exposed himself to me). To take a leaf from the post-war confessional prose by Martin Niemöller – “First they came for woman’s prisons, and I did not speak out because I was not a prisoner.”
Kellie-Jay Keen said in her speech “whatever steps you have taken, please take on step more”. Well, new gen Emmeline Pankhurst, this is my step. I have been personally undermined by trans ideology, and this is my story:
I am a 32-year-old Civil Engineer from Surrey. I have a wonderful husband and daughter, who was born last year. When I was a young girl, I was diagnosed with congenital breast asymmetry – a condition that predominately reveals itself at the onset of puberty. The cause of this condition is unknown, but it is has been linked to breast disease, developmental issues or hormonal problems. At 13 years old, my left breast was a non-existent AA cup whereas my right was a C cup respectively, coupled with irregular growth in my nipple and areola areas. I was under the care of a wonderful female doctor who immediately referred me to see a specialist at The Queen Victoria Hospital in East Grinstead, a hospital made famous in the War by the work of Sir Archibald McIndoe.
My mother and I met with Consultant Plastic Surgeon Mr. R W Smith, a gentleman who is famed for his work for burns victims and facial reconstruction. He advised us that I would likely have to undergo breast augmentation surgery to restore the aesthetic of my natural breasts. At the time, it was made very clear that to me that this procedure was a medical intervention, not cosmetic one. Admittedly, I was a little scared…however; the sting of pubescent self-esteem was starting to creep in and my relationship with my body image had already begun to deteriorate. I had started changing for PE in the toilet instead of the communal changing rooms. I knew something had to be done.
I was put on the waiting list for my surgery and in the interim was given a specially made gel prosthetic to wear in my bra. I was delighted. My confidence grew leaps and bounds and I started to attend more social events with my friends. Eventually my name was called and my surgery was scheduled during the school summer holidays before my 15th birthday. As a minor, I was placed in the children’s ward. The bilateral breast surgery was successful and I began the slow and very painful road to recovery.
Now a fun fact about ‘Top Surgery’ that the likes of Stonewall will not tell you is that there are actually two parts to it. Two goes under the knife. There is absolutely no medically conceivable way that a surgeon can just “shove” a breast implant into a patient who does not have enough skin to accommodate it. The first surgery is to insert a temporary breast implant, which is akin to an empty silicone bag called an ‘expander’. The implant is fitted in conjunction with a plastic port that is positioned just below your armpit so that the surgeon can access it at a later time. The implant is then filled with saline via a syringe directly into the port. Once the skin on your breasts has very slowly been stretched, the temporary implants are removed and replaced by the permanent set. This process took an agonising two further years to complete, but finally by 16 I had for the first time in my life a pair of natural looking breasts that I was very happy with.
The lifespan of a breast implant is 10-15 years; however, a common complication that can arise from such an invasive surgery is Capsular Contracture. This is where the scar tissue that naturally covers a foreign object in the body begins to thicken and slowly tightens around the implant. This becomes increasingly painful, the shape of the breast begins to distort and becomes hard to the touch. There is a medical grading for capsular contracture called the Baker Scale (1-4) which indicates to plastic surgeons when the implants require replacement. Unfortunately, my right breast began to show signs of this complication when I was 21.
I arranged to see Mr. Smith for a further consultation and was advised that the contraction in my breast on the baker scale was at Grade 2 and thus required replacement. Again, I underwent a further surgery to revise the breast and went about my life. A short while after this Mr. Smith retired from The Queen Victoria Hospital and I was placed into the follow up care of his registrar Consultant Plastic Surgeon Mr B S Dheansa. I have been a patient of his ever since.
I was unlucky enough at 26 to be plagued with another episode of Capsular Contracture on the same breast. Fortunately I knew the drill by now, and could spot the symptoms easily – a hardening of my right side breast and a slight discomfort. Naturally, I arranged to have an annual check-up with Mr. Dheansa to relay my concerns. On this occasion however, he informed me that NHS funding had since been severely cut for Women’s Breast Care as it was now deemed cosmetic in nature. To perform any surgery he would have to apply for funding on my behalf. He assured me that given my medical history and the fact that I was born with the health issue, he was confident that the surgery would be approved. The NHS gave me the implants in the first place – surely, they would follow up on any naturally arising complications?
A few months later, I received a letter from South East CSU and was informed in bold capital letters: FUNDING DENIED. As you can imagine, both my surgeon and I were aghast.
The letter went onto explain that unless the patient suffers from a rare or exceptional condition, no surgery could be undertaken regardless of any discomfort and/or if the implants were once clinically necessary. According to the NHS my breasts are now a cosmetic luxury, despite them causing me a great deal of pain. At the time of the initial denial, I was at the Baker Scale grade of 3.
Mr Dheansa has applied for funding on my behalf every subsequent calendar year, and each time it has been denied. I am now at the Baker Scale Grade of 4 which is classified as ‘hard, markedly painful to the touch and appears abnormal’ and I can attest to the fact that yes – I am in pain all of them time. Imagine having an elastic band inside of your breast, which with every given year gets pulled tighter and tighter to the point that you wake up in the night in a cold sweat, unable to breathe. You can no longer touch it in either a casual or sexual capacity and have difficulty putting on clothes. I was unable to breastfeed my daughter.
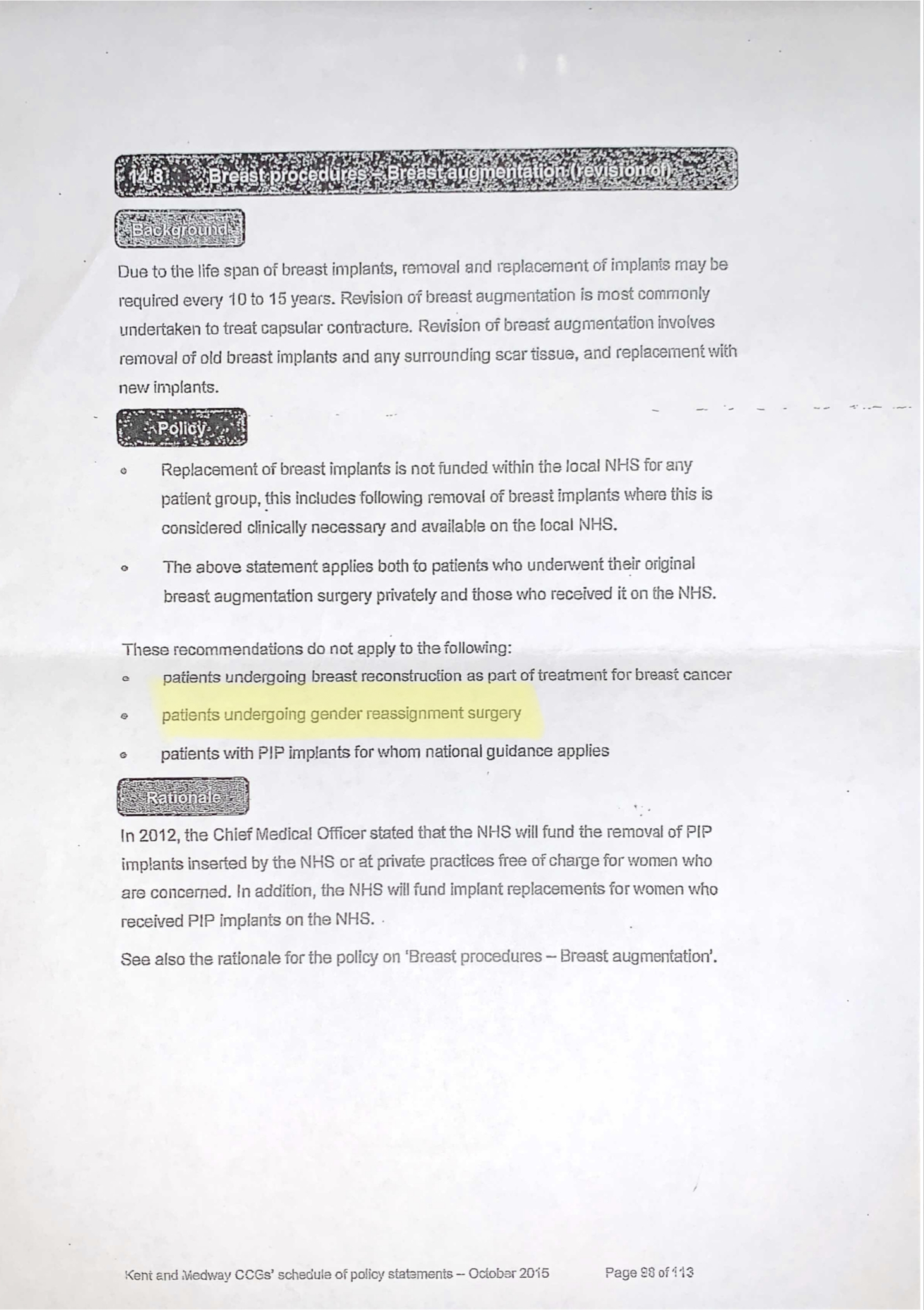
Despite all of the above, the greatest insult to me as a woman during these last few bitter years is the policy rationale as to why this service to women has been withdrawn, and to whom the recommendations for funding still applies to, these are as follows:
1. Female Patients undergoing breast reconstruction as part of treatment for breast cancer.
2. Female Patients with PIP implants for whom national guidance applies.
3. Male Patients undergoing Gender Reassignment Surgery.
Yes, you read that correctly. A man who wishes to have breast surgery as part of his gender affirming care is now more eligible for funding to make his non medically necessary, dysphoria induced dreams come true over my, a natal woman’s, need to have a congenital issue resolved. All I can say is thank heavens that the NHS still accept breast cancer survivors and the recipients of dangerous implants as a priority – but you never know, soon this too may be recognised as a luxury cosmetic procedure!
The only lifeline that has been afforded to me of late is that my surgeon has kindly offered to perform the necessary surgery that I need privately at a significantly discounted rate. “Then they came for women’s health care services” But I am speaking out now. Women’s breast care services should be afforded first and foremost to women, just as Urology is exclusively for men’s health. I am fed up of being on the receiving end of having my actual health needs ignored for the sake of validating men who merely want to look ‘like’ a woman.
This is happening. This is real. I have attached a selection of my medical letters, which I am happy for you to read.