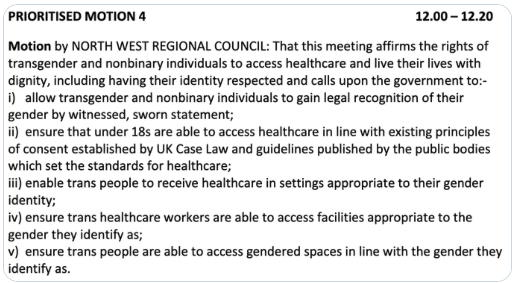
Two days ago, at the annual meeting of representatives which had “diversity” as its theme, the British Medical Association (BMA) passed a motion to endorse gender self-ID for both healthcare staff and patients, and to campaign for them to have access to gendered spaces in line with the gender they identify as.
You might think that this motion had the benefit of prolonged debate where all the members were informed of the issues and allowed to contribute, but you would be wrong. Most BMA members I know personally haven’t even heard of this motion, and those who were present told me that the chair of the meeting declined requests for postponement and allowed only 20 minutes for the discussion before it was put to vote. In the end, out of 159,000 BMA members, around 125 delegates voted (out of 250 that were present), and the result was split 49% for the motion and 36% against, with a substantial block abstaining from voting.
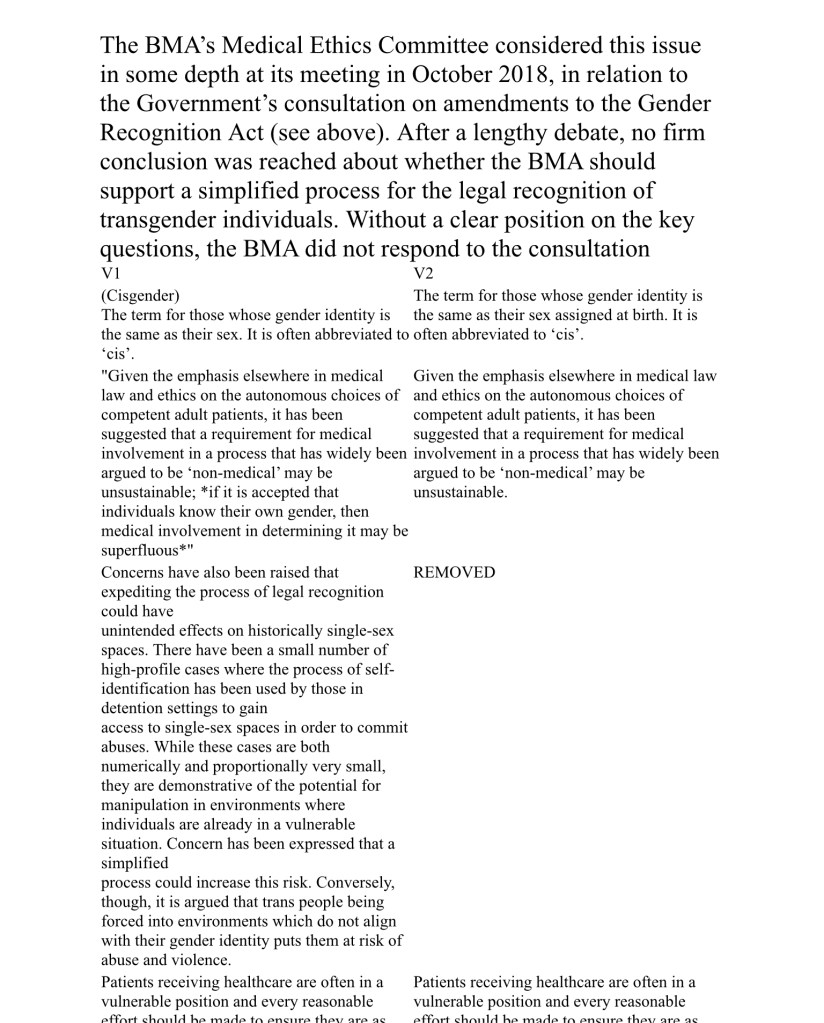
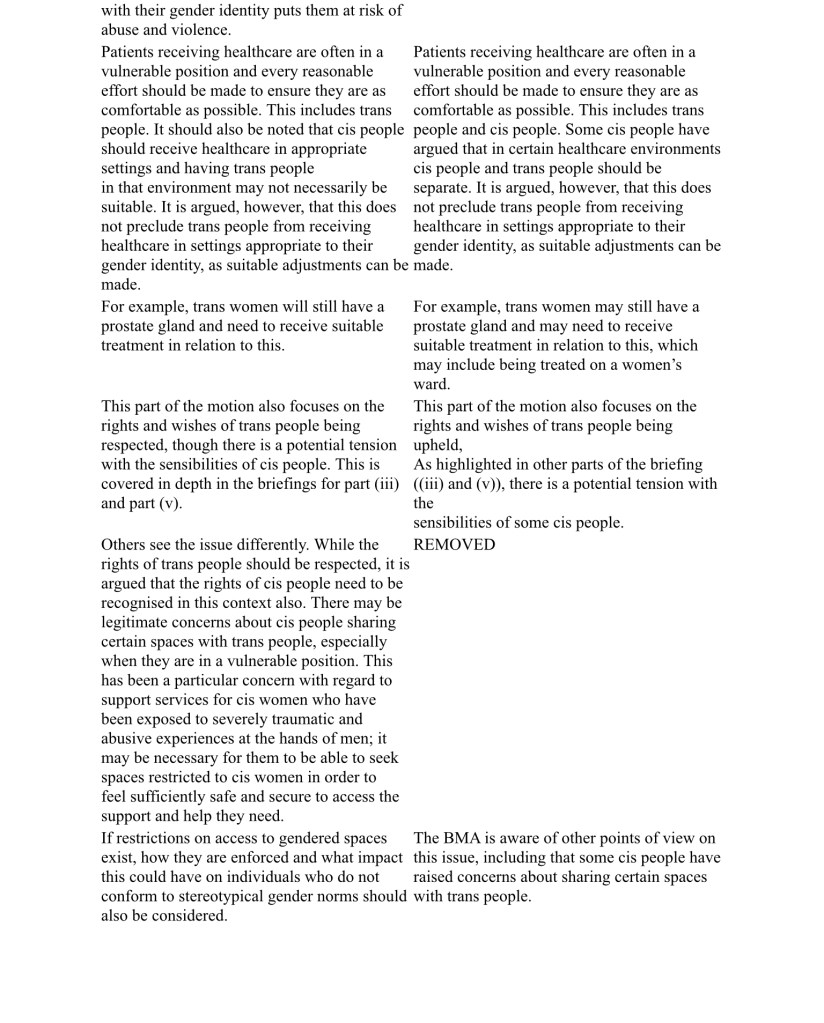
To be fair, there was a brief (V1) about this that was published in advance. However, this brief was removed, allegedly on advice of the BMA lawyers, and replaced by a second brief (V2) which was distributed before the vote. In the screenshots below you can see that the second brief V2 had all discussion about the impact on women’s sex-based rights removed, and replaced by facetious statements such as that “there’s a potential tension with the sensibilities of some cis people”.
What sort of debate on a serious and wide-reaching issue such as this can possibly be had in 20 minutes, one might ask? The BMA thankfully provided us with a few key examples.
Opposing this motion, Dr Angela Dixon focused on ethics, evidence-based medicine and the Equality Act 2010.
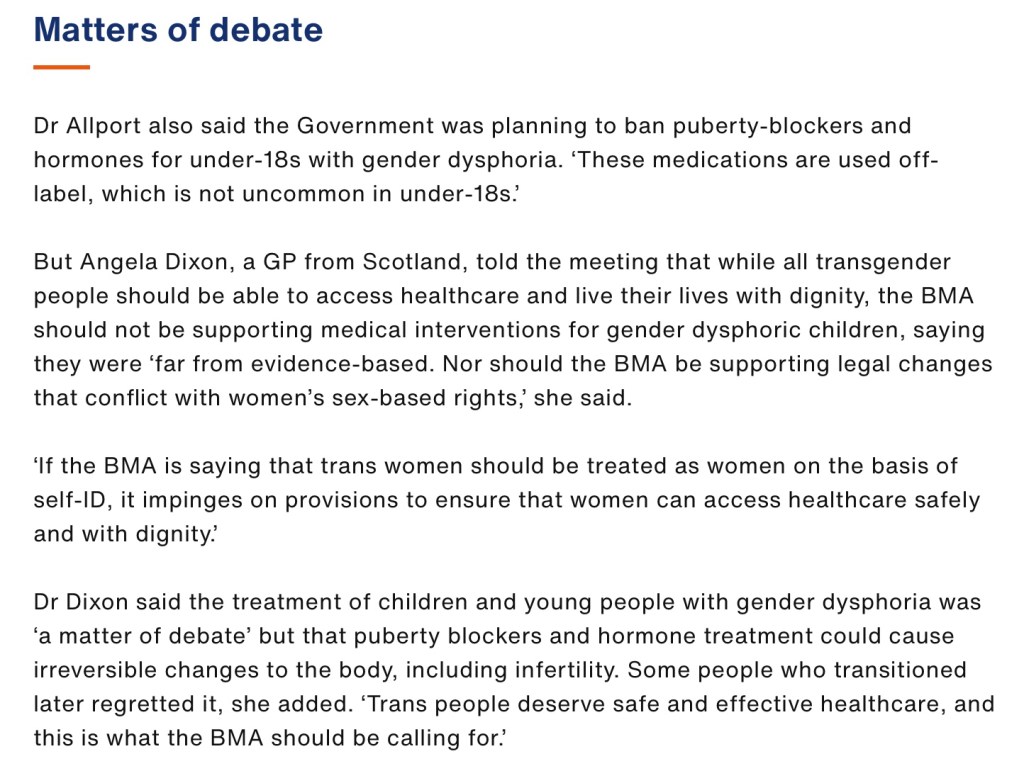
Dr Allport argued for gender self-identification:
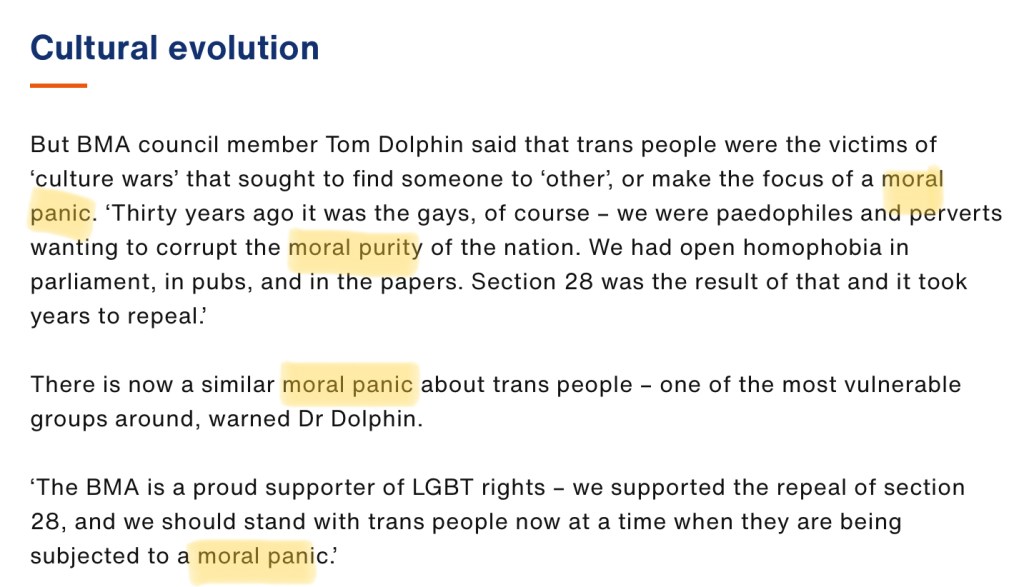
While Dr Tom Dolphin insinuated that women’s sex-based rights were rooted in “moral panic”, a term he kept repeating during the debate and later on twitter, where he muted those who asked legitimate questions and referred to them collectively as “transphobes”.
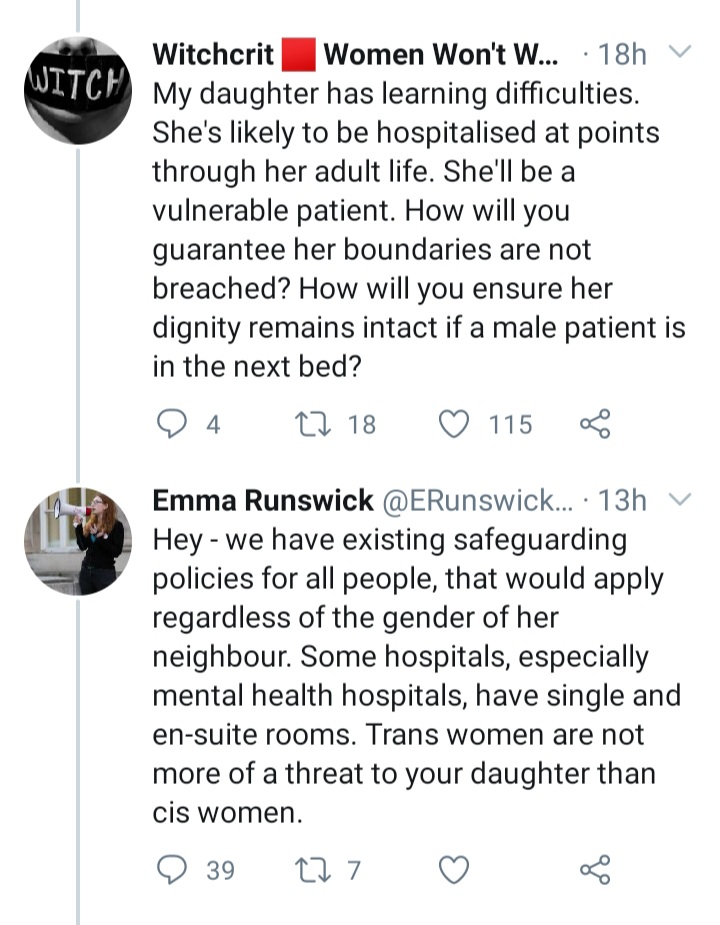
On twitter, we also heard from another BMA delegate who supported the motion. A newly qualified junior doctor Emma Runswick initially informed us that she was delighted the motion had passed, that she worked hard to see it come to fruition and that she welcomed questions about it. However, it quickly became apparent that Emma had poor understanding of the issues involved, such as in this case where she falsely reassured a concerned parent of a vulnerable child that “transwomen are not more of a threat to your daughter than cis women”.
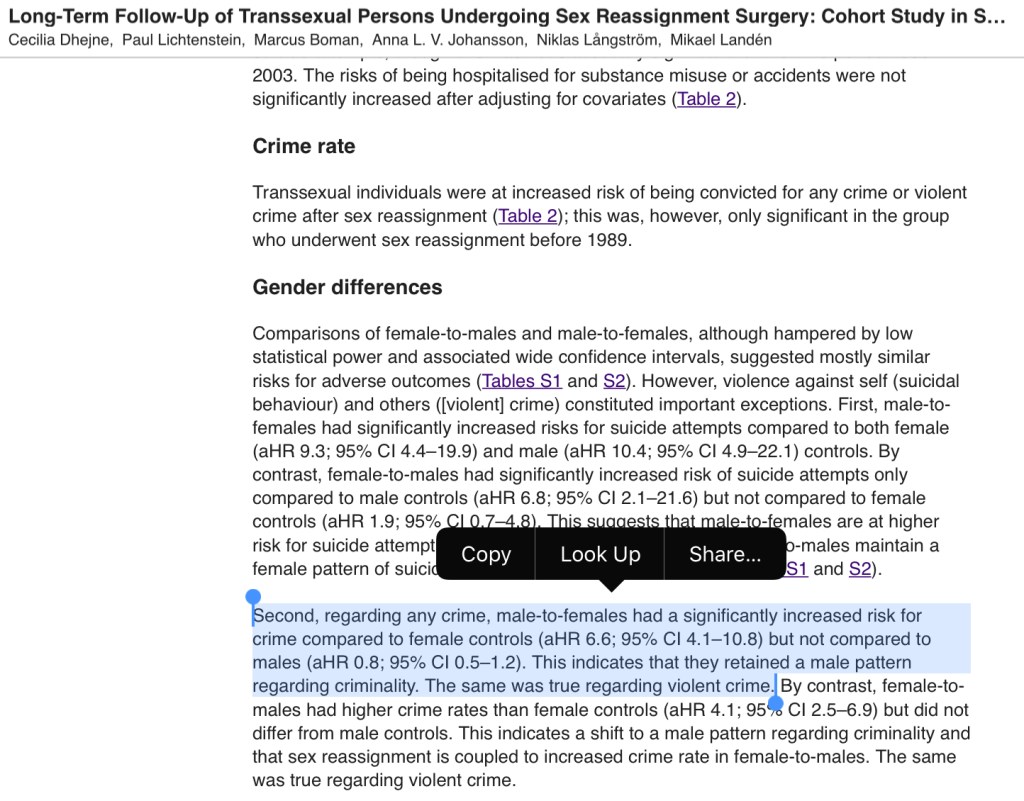
In reality, the biggest long-term follow up study on gender reassigned individuals we have available has shown that transwomen offend at the same rate as other males, and MoJ’s own figures show that roughly half of transgender inmates in UK prisons are sex offenders.
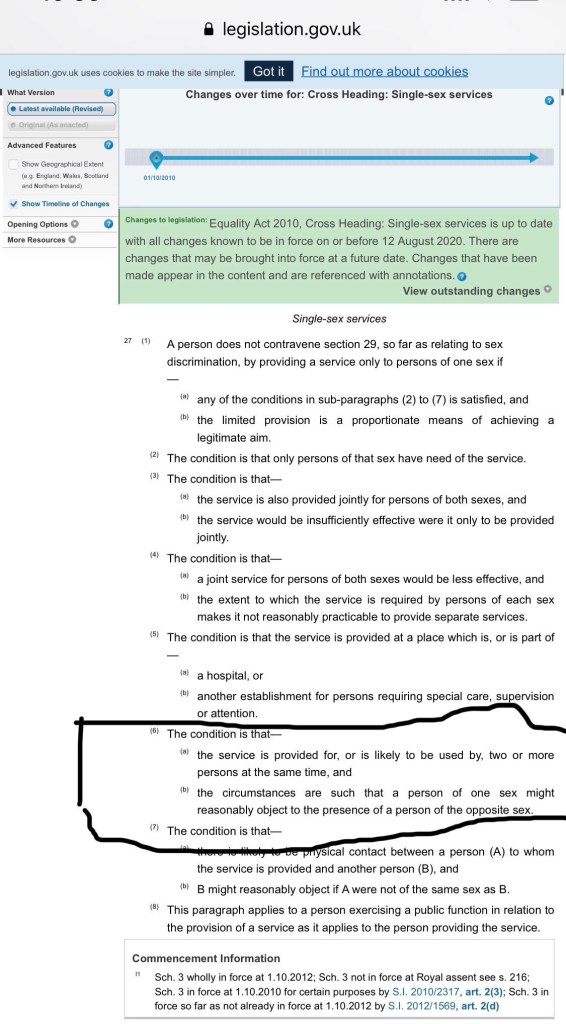
Having failed to adequately explain and support her position on twitter, Emma blamed those who questioned her and closed her thread for comments. She also claimed that the definition of a lesbian, which literally means “a homosexual female” or “female who is exclusively sexually attracted to other females”, is “phallocentric”, and didn’t seem to realise it was her who was misunderstanding exemptions under the Equality Act 2010, which in no uncertain terms specify that even males who hold Gender Recognition Certificates (protected characteristic of “gender reassignment”) can be lawfully excluded to provide single-sex services to females.

I really don’t want to put all this on Emma though. I have tried to converse with her on twitter but she ignored me, so I was unable to clarify her attitudes and beliefs. But it strikes me as typical of male misogynists to put forward a young and inexperienced female to do their dirty work. Despite her indignation at being called young/naive by older women and female colleagues, this appears to be the explanation for much of her conduct. Be it as it may, she has been instrumental in legitimising this policy so she deserves a mention.
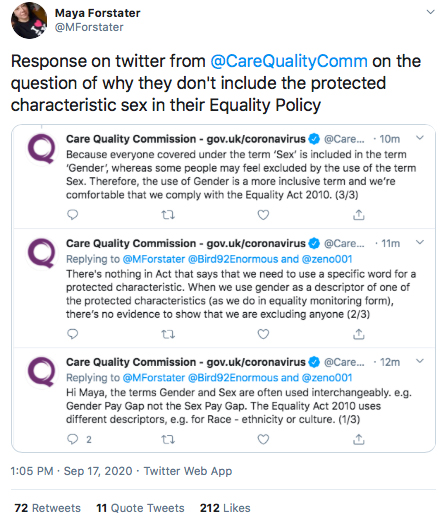
Another organisation that deserves a mention is the Care Quality Commission, the regulator of health and social care services. When Maya Forstater, who recently published the article “Trans healthcare professionals and patient consent” in which she examined the medico-legal implications of male doctors being allowed to self-identify as female, asked the CQC why they replaced “sex” (protected characteristic) with “gender” (not a protected characteristic) in their Equality policy, the CQC claimed that “there was nothing in the [Equality Act 2010] that says we need to use a specific word for a protected characteristic”.
Imagine that! So I suppose we can replace “age” with “apples” and “disability” with “oranges” and make any old word salad out of the law :shrug:
Having reviewed all this evidence, however, I am struck by how closely this follows strategies outlined in the report titled ‘Only adults? Good practices in legal gender recognition for youth’.
I have no information about the demographics of BMA representatives who were present at the meeting, but both representatives who promoted this motion on social media, Emma Runswick and Tom Dolphin, were young and political.
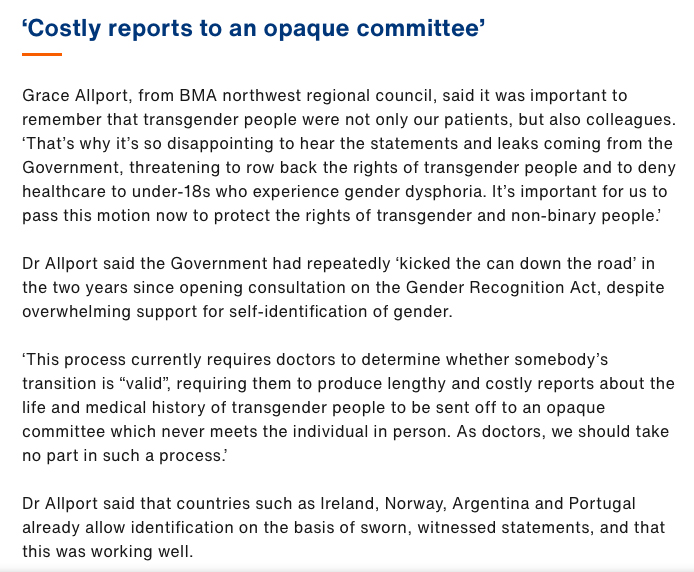
Dr Allport has argued (Fig. 6) for de-medicalisation of gender recognition by saying ”This process currently requires doctors to determine whether somebody’s transition is “valid”, requiring them to produce lengthy and costly reports about the life and medical history of transgender people to be sent off to an opaque committee which never meets the individual in person. As doctors, we should take no part in such a process.”
She also encouraged the BMA to get ahead of the government and publish progressive legislative proposal before the government had time to develop their own by arguing that “the Government had repeatedly ‘kicked the can down the road’ in the two years since opening consultation on the Gender Recognition Act, despite overwhelming support for self-identification of gender”, a claim which is more hotly debated in the UK than even Brexit, and isn’t supported by official data.
This motion was framed in terms of human rights of trans and nonbinary people, while the evidence of the motion’s negative impact on human rights of women was removed from the brief (Fig. 3,4), and it was tied to a more popular reform of “diversity and inclusiveness” while Tom Dolphin made repeated parallels with Section 28. The motion certainly managed to avoid excessive exposure and coverage, so much so that most members weren’t even aware of it, while “carpe diem” was enacted literally, by denying requests for extension and pushing the motion through on the same day.
But there’s another point in Denton’s report which can be found on p.19 – 3. Use case studies of real people. I would like to talk about that now.
When I first heard of this motion being passed, I offered to speak to the BMA, as a doctor and a rape survivor, about the impact this policy will have on women.

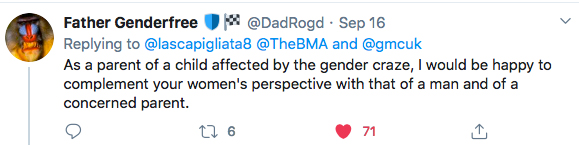
If you read the comments under my tweet you will find many others, trauma survivors, doctors, disabled women, teachers, parents of disabled and ROGD children, joining in and offering to speak to these institutions as well.
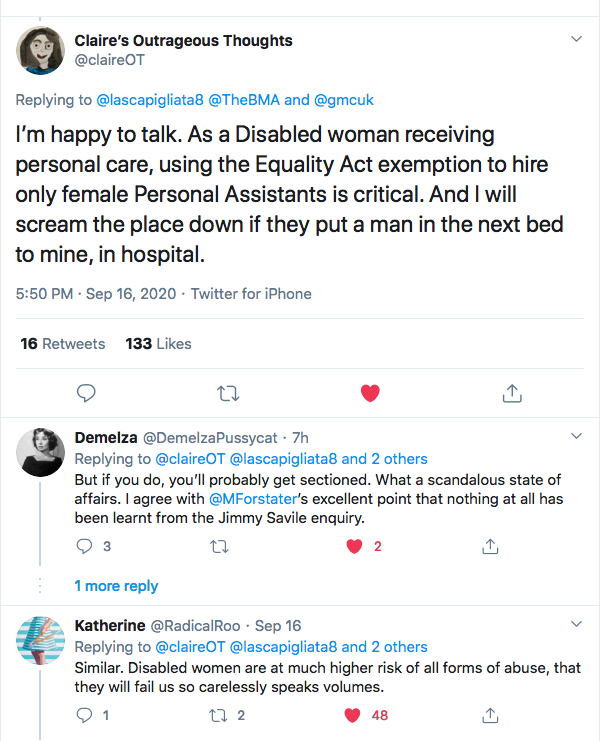
Some women offered personal testimonies of either suffering or witnessing sexual assault by a male in a healthcare setting.
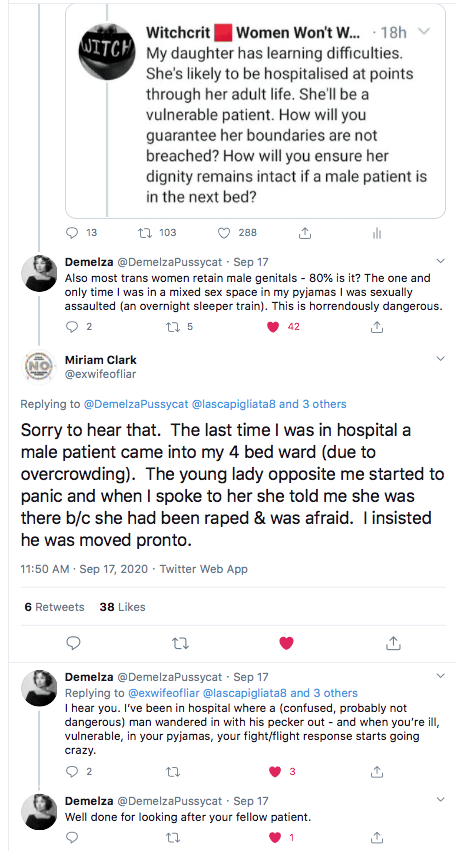
Other shared news stories, such as this one where a 17 year old girl was raped in an all-male hospital room in Ireland, a country where according to Dr Allport (Fig. 6) gender self-identification was “working well”.

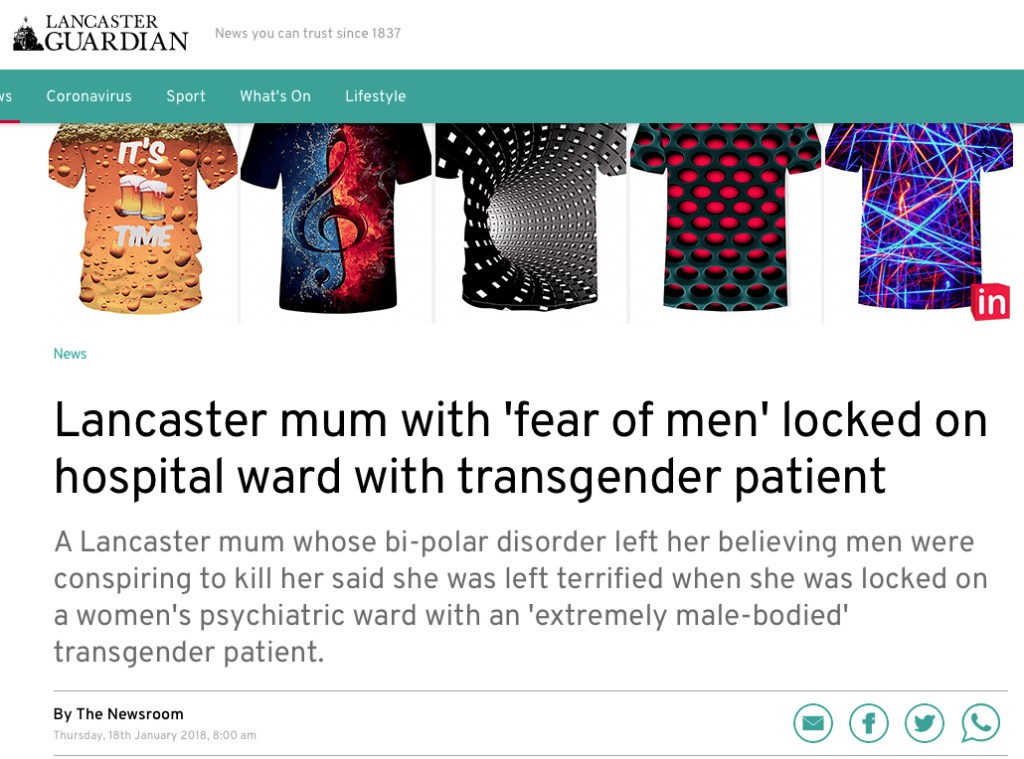
And this one about a patient who was sectioned during a manic episode and was gaslighted by the staff on the psychiatric ward that a male patient was really a female and was labelled a “transphobic bigot” in the medical notes.
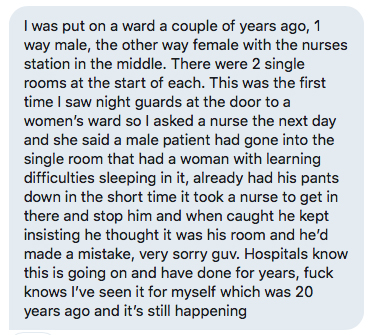
And this one, presented without comment:

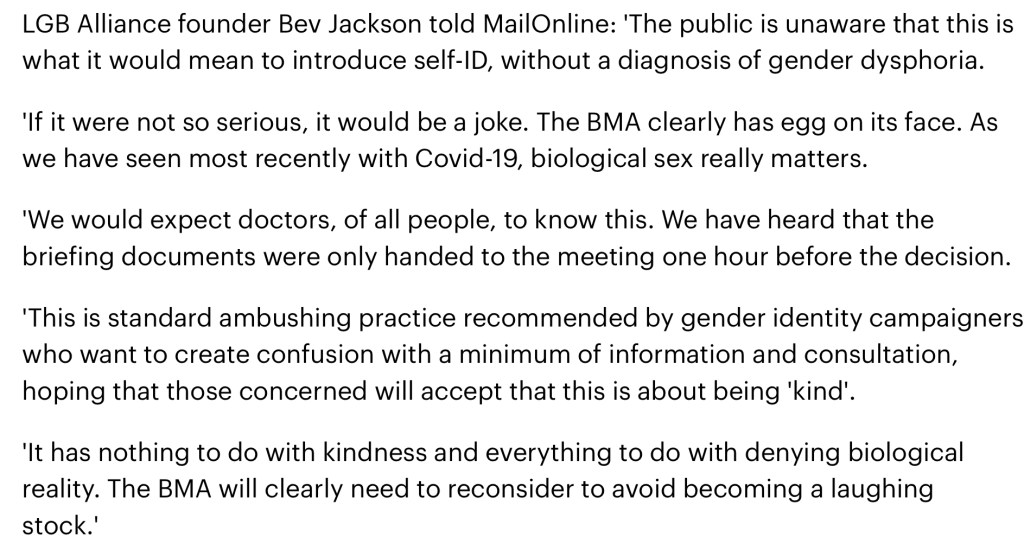
It’s been three days and we have not had any response from the BMA’s social media account. Many who have written to the BMA directly got rebuffed with the same dubious arguments that were heard at the meeting. Members have started cancelling their BMA memberships. Members of the public have expressed concern and disbelief at the process and the motion itself. Bev Jackson, the representative of LGB Alliance, a UK group who campaign for the rights of gay, lesbian and bisexual people, warned the BMA against “denying biological reality” and becoming a “laughing stock”.
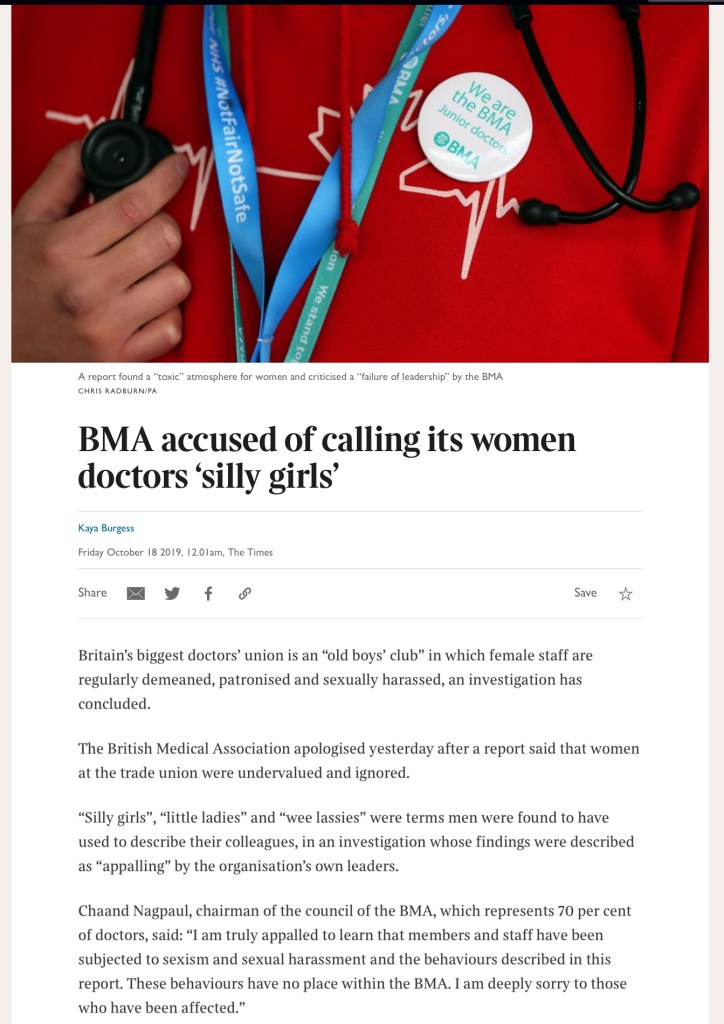
As we waited and waited, the conversation naturally turned to the deeply entrenched sexism and misogyny within the BMA and, more broadly, in the medical profession.
Leaving this here for posterity.

I wish women could wear a body cam, like cops are supposed to these days, so they’d at least be able to prove they’re not making up false accusations against men when they’re simply describing what a woman’s normal existence is like.
LikeLiked by 2 people