(NOTE: I will start with introduction to the issues. If you have heard all this before, please scroll down to see the examples.)
For over a decade, UK institutions were given erroneous advice on the interpretation of the Equality Act 2010, specifically relating to the protected characteristics of “sex” and “gender reassignment”.
The errors typically include:
Replacing protected characteristic of “sex” with “gender”.
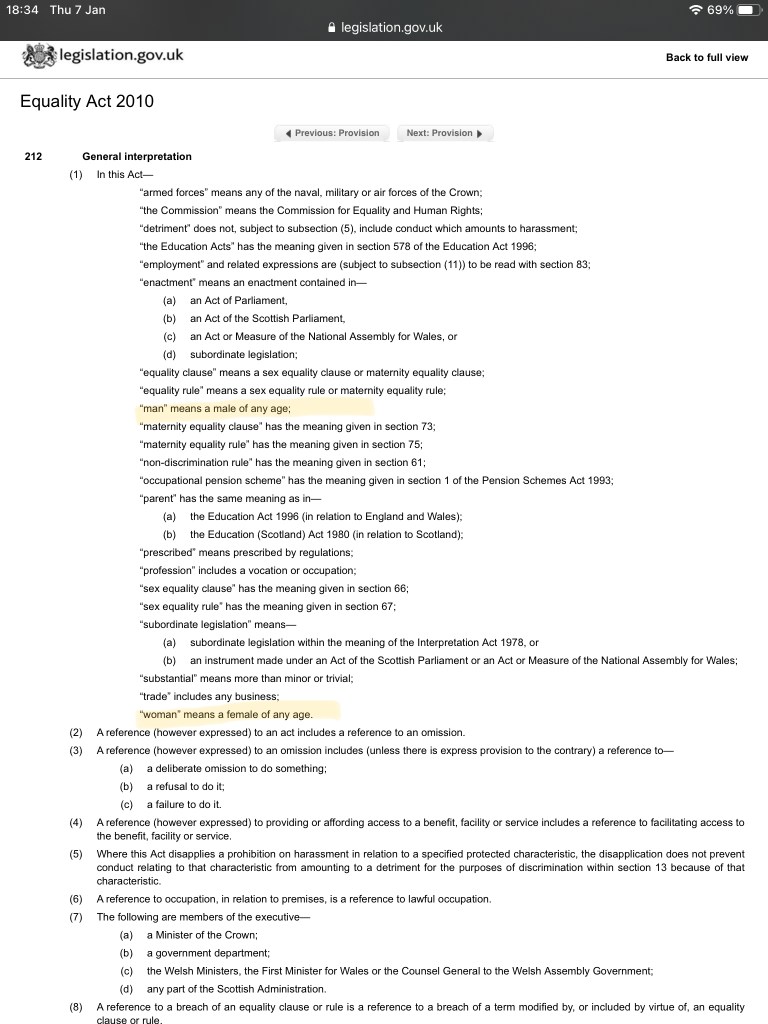
Sex is clearly defined in UK law, for example legally, woman is defined as “a female of any age” under the understanding that words “female” as well as “male” refer to humans and are understood to mean the two biological sex classes needed for sexual reproduction.
Meanwhile, word “gender” isn’t clearly defined. Originating as a linguistic term, it was used by a sexologist and father of “gender reassignment” John Money to mean sex role stereotypes of masculinity and femininity. Over time, “gender” has crept in by convention as a “more polite” word for biological sex, but this has never been formalised in law, or science or medicine.
Replacing protected characteristic of “gender reassignment” with “gender identity”.
In UK law, Gender Recognition Act of 2004 was brought in to allow creation of legal fiction – change of sex marker on birth certificates and medical records – for people who have undergone medical transition to change their bodies to resemble the opposite sex. This was needed in order to give legal rights to transsexuals in context of same-sex relationships, given that same-sex marriage was not legal in the UK at that time.
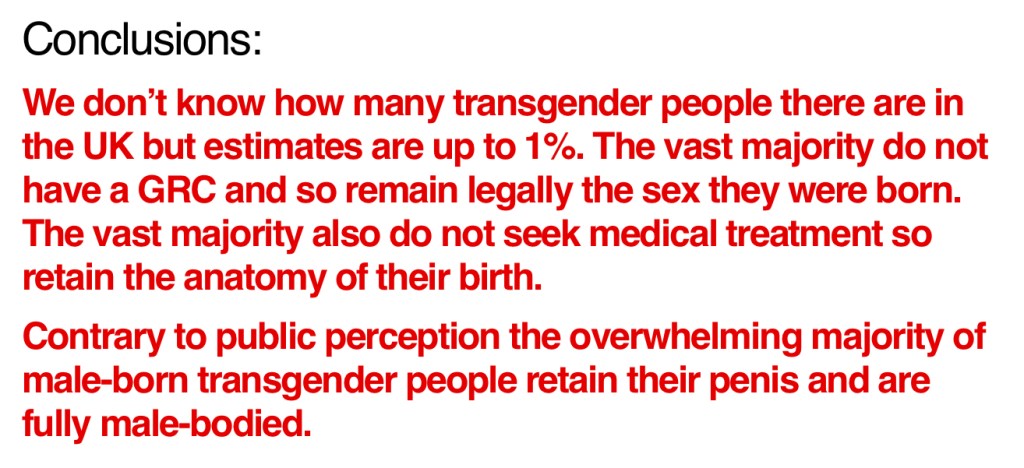
This legal fiction is facilitated by Gender Recognition Certificates, which are given to people after two years of psychological assessments and evidence of living in the role of the opposite sex. Genital surgery was never a requirement for obtaining a GRC, and evidence shows that vast majority of transwomen retain their male genitals.

On the other hand, “gender identity”, like “gender”, is a non-specific term that isn’t legally defined, but it’s come to mean “internal sense of being male or female” and this has formed the basis for claims such as that “transwomen are women” and “transmen are men” and that to deny these statements amounts to a hate crime of “transphobia”.
From the beginning, GRA legal fiction generated changes of sex markers to wrong sex on patient medical records, but trans status tended to be clearly flagged up. Individuals who obtained the GRC did so under the understanding that biological sex is important and should not be concealed. Also, the fact that “passing” as the opposite sex was actually rare, and that medical professionals were allowed to freely inquire and discuss it, meant that the potential for medical mistakes was reduced.
It has to be said that the goal of the GRA and GRC was never to conceal or erase sex in language, law, education or medicine, but to reduce discrimination toward transsexual individuals and to make administrative aspects easier for them. To this end, the GRA specifically states that this legal fiction doesn’t actually change biological sex, women can’t transition to men in order to claim primogeniture (inherit aristocratic titles for example) and subsequently under the exemptions to the Equality Act 2010, male holders of GRC can be lawfully excluded from women’s single-sex spaces.

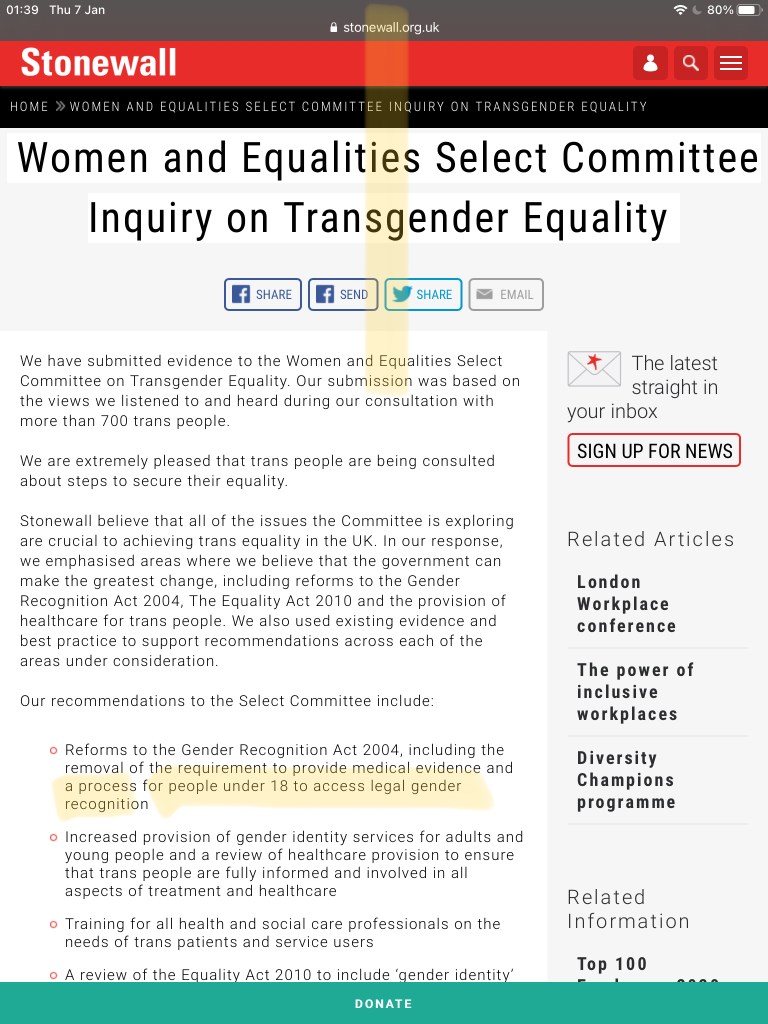
However, since GRA was brought in, the LGB organisations such as Stonewall UK rebranded themselves as LGBT+ to include “transgender” (loosely defined umbrella term that includes anyone who doesn’t conform to gender stereotypes, including transsexuals and crossdressers) and started to campaign to amend Gender Recognition act to remove medical gatekeeping for GRCs, to allow anyone to self-identify as the opposite sex, to give children access to medical interventions designed to irreversibly alter their bodies with puberty blockers, cross-sex hormones and body modification surgeries, and to remove single-sex exemptions, ie. to remove women’s legal right to single-sex spaces and service provisions.


Almost every institution in the UK, including hospitals, NHS Trusts and universities, has signed up to “champion” these goals, by participating in Stonewall Champion scheme.
Please see the extraordinarily long list of Stonewall Champions here
Eventually, and despite the fact that there is no scientific evidence of biological basis for gender identity , through combination of misinterpretation of the law and NGO campaigning on the platform of “Acceptance Without Exception”, legal fiction has nonetheless come to trump the reality of biological sex in practice. Since these misrepresentations have been allowed to run rampant in UK institutions, we have witnessed disappearance of all women’s single-sex spaces, from hospital wards, prisons, DV and rape crisis shelters to women’s shortlists, public toilets and changing rooms. And increasingly we are seeing hospitals implementing “trans-inclusive policies”, which are designed to ensure should a woman complain about presence of a man in what is claimed to be a single-sex space, she is sooner accused of transphobia and bigotry than listened to and given the benefit of her legal rights.
This brief twitter exchange with a doctor involved in championing LGBT+ causes speaks for itself:



I won’t be commenting on any specific treatments in this article, such as experimental interventions on gender dysphoric minors, but if you haven’t already, please read about the current situation where UK High Court has deemed children under the age of 16 incapable of consenting to irreversible changes to their bodies in Bell vs Tavistock Judicial Review.
So without further ado, let’s take a look at some examples.
General Medical Council (GMC)
Patients can no longer depend on the medical regulator to truthfully inform them of a doctor’s biological sex. They allowed change of name and gender *without any evidence*. Just fill an application and GMC will give a different set of details.



As Maya Forstater explains in her excellent article:
“There is no national approach to transitioning at work in the NHS, but regional trusts often have policies (For example these ones from West Suffolk, Cambridgeshire and Peterborough, Brighton and Sussex). The NHS trust policies are all slightly different but cover similar “acceptance without exception” ground, following the recommendations of organisations like GIRES. I have not been able to find one which considers how accommodating the desire of some health care professionals to be treated as a member of the opposite sex at all times interacts with the rights of patients. This is a policy blindspot.”
GMC has also advised doctors that they should change patient’s “gender marker” upon request and likewise, no evidence of transition is required.

The procedure, as outlined by Public Health England and carried out by individual doctor surgeries, is outlined below:


The consequence of this on patients is nothing short of unethical.
“A Lancaster mum whose bi-polar disorder left her believing men were conspiring to kill her said she was left terrified when she was locked on a women’s psychiatric ward with an ‘extremely male-bodied’ transgender patient.
When she raised her concerns with hospital staff, however, she said she was not taken seriously and her medical notes implied that she was a “transphobic bigot”.”
British Medical Association (BMA)
Please see here for detailed analysis of recent policy capture that led the BMA to fully endorse self-identification of sex ie. mis-sexing by declaration.
The motion that was passed at BMA conference appears to uphold all Stonewall campaign points, including unrestricted gender self-ID for patients and staff, access to irreversible treatments for minors, and effective destruction of women’s single-sex spaces and healthcare provision.
Note their usage of the term “existing principles of consent”, which refers to claims that under 16s are Gillick competent to consent to medical transition. This has since been confirmed wrong thanks to Bell vs Tavistock ruling.

Care Quality Commission (CQC)
When CQC were asked why they replaced “sex” (protected characteristic) with “gender” (not a protected characteristic) in their Equality policy, the CQC claimed that “there was nothing in the [Equality Act 2010] that says we need to use a specific word for a protected characteristic”.

MEDICAL EDUCATION
In the UK, apart from the teaching hospitals and universities being signed up to Stonewall Champion scheme, medical schools are also members of Athena SWAN award scheme.

Athena SWAN was originally meant to address inequality of women in STEM, and despite the fact that they too are using “gender” as a more polite word for “biological sex” their pages mainly talk about equality of “women” and “females”. They also correctly include “sex” and “gender reassignment” on their lists of protected characteristics, but some universities have already altered these to “sex/gender”.

When you dig deeper, you will eventually encounter the following on Athena SWAN website:
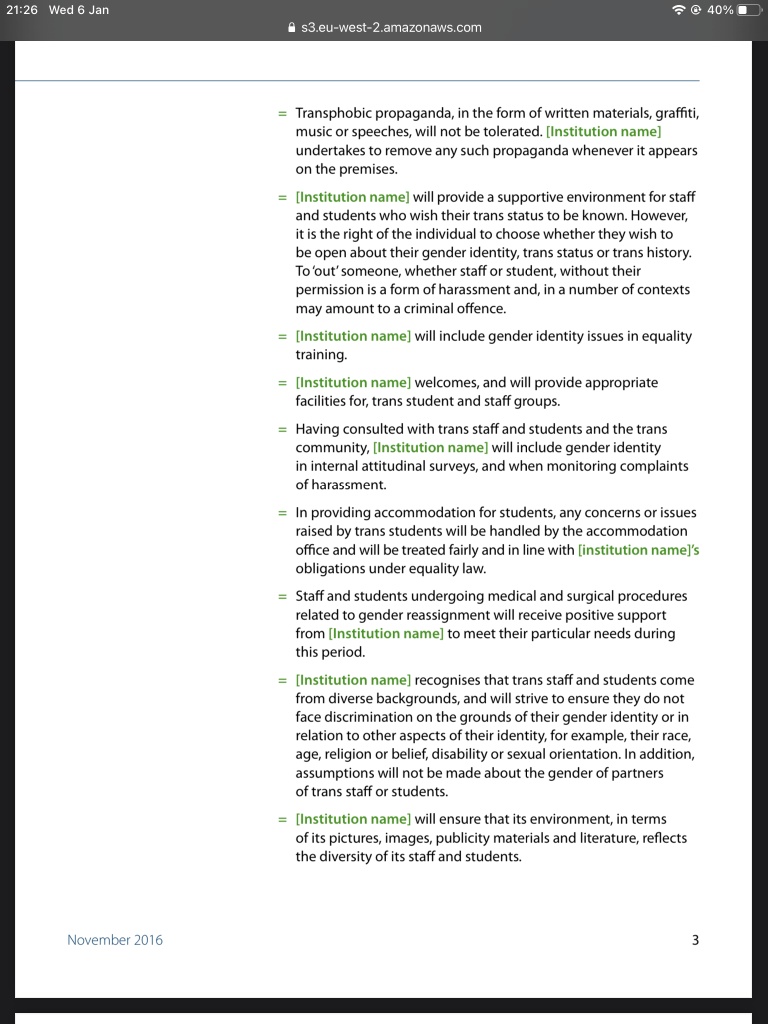
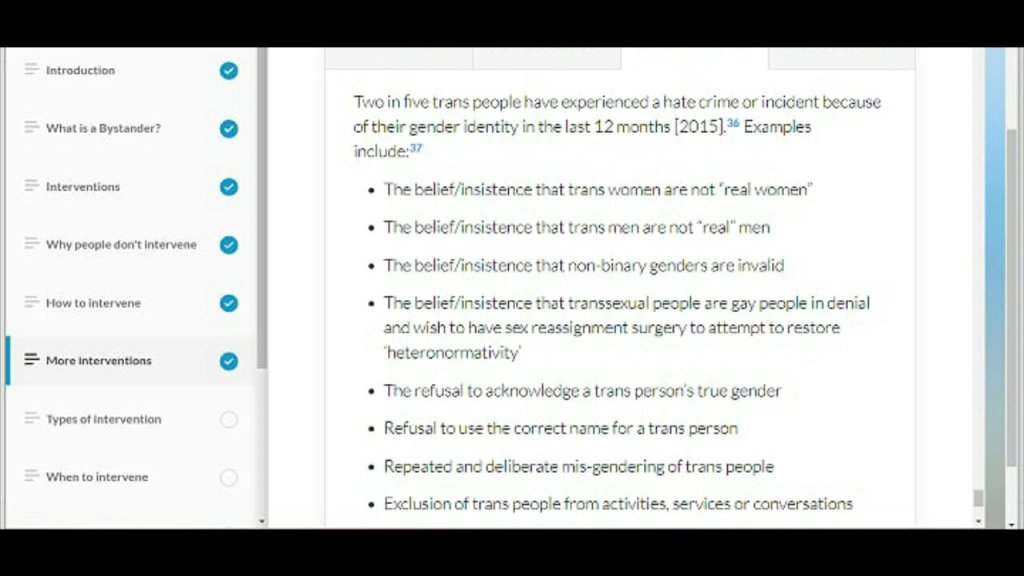
“Sex assigned at birth” even though sex is observed not assigned. Replacing “sex” (observed) with “gender” (assigned, culturally) in the list of protected characteristics. Enabling de facto self-ID for students and staff, thus breaching single-sex provisions under the EA2010. Referring to “unwanted questions”, such as perhaps noticing a person’s biological sex, as “transphobic abuse” and attempts to discuss it as “transphobic propaganda”.



So it’s hardly surprising that medical students are reporting that they are compelled to undergo training about “hate crimes” and told they could be kicked out for “inappropriate behaviour” which, according to the modules, includes “belief/insistence that transwomen are not real women”.
One thing that quickly emerged in my enquiries is that medical students, professors and and doctors alike are all very reluctant to be found to oppose, question or complain about the diktat of gender ideology. Therefore, some of the following examples, which come from all over the English speaking world, were shared with me on condition of anonymity.
“Oh it’s quite crazy over here! I’d rather not divulge the precise location but I can say it is an upper tier school with heavy involvement in research and teaching. Most of the wildest wokeness tends to be centered around race and gender – specifically, transgender ideology.”
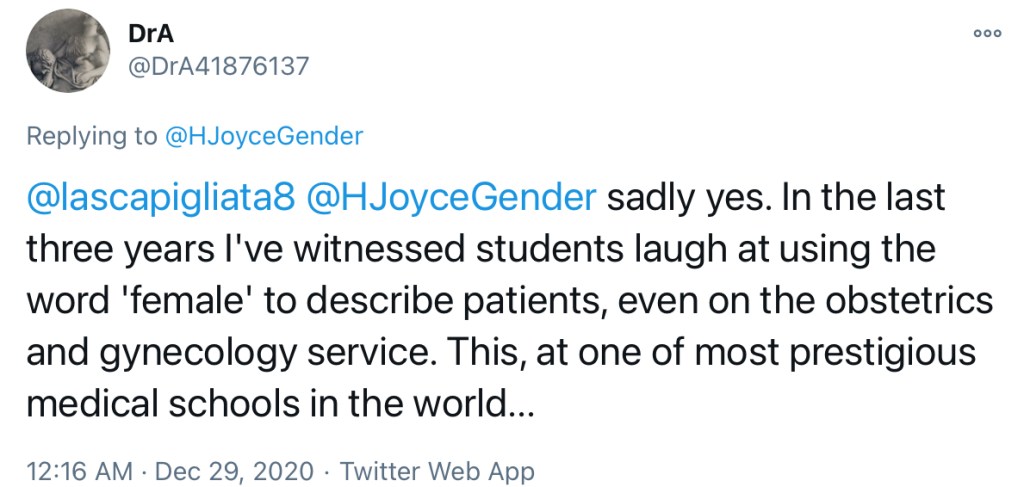
“In the last three years I’ve witnessed students laugh at using the word ‘female’ to describe patients, even on the obstetrics and gynecology service. This, at one of most prestigious medical schools in the world…”
“In a journal club, when our group was drafting a problem statement for our patient (a girl [… ] with sickle cell disease”, we wasted over 5 minutes debating whether it was appropriate to allude to the patient’s sex in our opening statement. I argued that it was potentially relevant (I’m not a sickle cell expert, but I suspect that sex might have some influence on disease severity), but the vocal minority in my group argued that “we can only infer the patient’s gender identity through her pronouns, we can’t infer her assigned sex at birth, so we should just leave it out”. And keep in mind, all these examples are from “bread and butter” science classes. NOT the woo-woo gender identity materials and race relations workshops through which we also had to suffer.”
“If any socially liberal/woke people ever try to say, “Well, no one actually is saying that sex isn’t real, they’re just saying that gender is fluid”, they are lying or misinformed. I was told this information on many, many separate occasions.”
“I’m in med school, and I shit you not, this slide came up in one of our class presentations:”

“I went on a course re inclusion of lgbt students, this was the main course material. It is also pinned to the wall in the Pastoral Lead’s office. Also Stonewall posters through the corridors.”

“A talk from a student at (Hull York Medical School) but was part of official medical school pride month events and platformed on the medical school’s social media pages.”
“In an anatomy lab where we were looking at a (disassembled?) pelvis/reproductive organs, I was asked “Would you like to see the assigned-female-at-birth or the assigned-male-at-birth specimen first?”
“Different prevalence of asthma between the sexes are “most likely due to the difference in average ribcage size and not due to the gender of the people” (a very bold claim)”
“It was implied in a lecture that the different rates of cardiovascular disease in men vs women are actually due *solely* to the higher presence of androgens “associated with AMAB people” and not “easily dividable by sex”. Oh, by the way, biological sex is a social construct. That made my jaw drop to the floor.”
“Many/most of the lecture and reader materials have been changed to say “AFAB” and “AMAB” or “XX individuals” and “XY individuals”, in lieu of female and male. Most of the instructors don’t seem to be super on-board with these distinctions but many are well-intentioned, trying to be polite/an “ally”. If anything, this makes them much more vulnerable to scrutiny. I’m not sure if it’s due to sexism or due to displays of weakness/appeasement, but the female professors who have committed Wrongspeak have been held to much higher scrutiny by my fellow uber-woke students than the male professors. we had a genetics professor who interchanged between using the terms “AFAB/AMAB” and “female/male” multiple times… in response, some of my wokest students drafted a 5-7 page letter outlining every one of her “crimes” and sent it around our class’s Slack channel to get it signed and sent to the Deans so she could be encouraged to “do better” (ugh). I can recall there or four other petitions circulated for similar reasons, all related to similar instances.”
“I’m seeing the ideological indoctrination in my relative’s nursing program both in what is overtly taught and in passing time over to speakers who have no evidence backing their statements.”

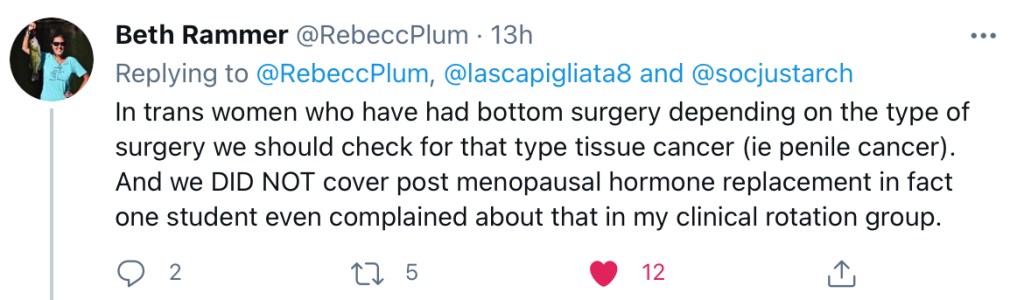
“During my OB/GYN didactic course for my masters degree. 1/5th of the course concentrated on trans women, that’s 20% of the course work focused on biological males, 0% on post menopausal women. Yet, my rotation (real life) 0 trans patients and 55% post menopausal women.”
“I should clarify that we also covered STDs during this course. (I just want to be as honest as possible). The first week of a 7 wk course was on inclusivity, how not every woman has a vagina….We were told we should not refuse to do a Pap on a trans woman….”
“In trans women who have had bottom surgery depending on the type of surgery we should check for that type tissue cancer (ie penile cancer). And we DID NOT cover post menopausal hormone replacement in fact one student even complained about that in my clinical rotation group.”


“I am a midwifery student. I have to use “pregnant people” in my papers or I get docked.”


In a sea of bad examples, there are some good ones. Such as:
“They have had one OSCE with a trans woman as the [patient] in their 3rd year . Where they were marked on the use of correct pronouns BUT expected to realise that medically it was important to note the sex is essential in treating the pt for certain conditions . So I guess it’s exactly what you would be hoping all medical schools are teaching.”
However, the overwhelming picture is one of students and clinicians operating in an environment saturated with gender ideology, as this testimony illustrates:
“I saw a transwoman in the ED the other day. Medical records all said ‘female’. NHS number was new. Nothing from [patient] to reveal natal sex, except ‘I take HRT’. I could see this patient was taking 6x the exogenous oral oestrogen normally taken post-menopause, plus a weekly patch. Formerly took [androgen blocker used in feminisation therapy for males] and had had NHS speech and language therapy.
With patient’s consent I viewed the SCR [Summary Care Records], to record drug history accurately in the notes. In the SCR natal sex was not recorded. All it contained was childhood immunizations and current drugs. No ‘diagnosis’ relating to drug history. No record of any surgery.
A few points.
If this patient was bleeding, I would send group and save. This would go to blood bank with sex erroneously marked as female. I’m not a haematologist but are there risks around this, I don’t know?
If the patient donated blood, is natal sex recorded?
Patient had [shortness of breath]/cough/chest pain. Was sent in for PE work-up, presumably because the massive doses of oestrogen are a big risk factor.
I did bloods, d-dimer, chest X ray etc.
Investigations were negative for PE but there was an incidental finding on chest x-ray of healed fractures with no history of trauma, which is unusual to see in a young patient.
I was concerned this might indicate reduced bone density, knowing this can be a side-effect of gender reassignment therapy. I discussed this with the patient, without at any point suggesting that I didn’t take patient’s recorded sex at face value. I thought it was in the patient’s best interest to mention the incidental finding in the patient’s discharge letter.
Anyway, I’m telling you all this because I suppose it highlighted to me a few things about how unhelpful it is from a clinical [point of view] to go down this gender rabbit hole. For the patient, passing and being dissociated from their natal sex is important. They are permitted to have a new name, NHS number and sex on their records. Their wish/need for gender affirmation is prioritised over their clinician knowing something as fundamental as their sex when it comes to diagnosing and treating them.
Also, the current climate means that, presented with a patient like this, I can tell you I was nervous as hell about saying the wrong thing. I’m not talking about misgendering, it’s easy not to do that… What I mean was that I was terrified of saying anything that hinted I’d observed or considered that the patient might be a transwoman, in case I upset them or attracted a complaint.
There was lack of candour and openness, and waryness on both sides, which is not conducive to delivering best clinical care to the patient.
Prior to this encounter I was unaware you could change both your sex and NHS number on your records. I looked into it and I found a discussion on Reddit between some young trans individuals who were exchanging information about how to get a new NHS [number] changed (from what I remember it is easy and I’m not even convinced you need a GRC).
What was also clear, is that their priority in getting new NHS number is so they can actually hide, erase, their sex… it’s all about passing.”
More worryingly, serious medical errors have already occurred, all affecting trans-identified patients. Please read my analysis of a case whereby a transman was denied renal transplant because medical team kept using male equations to calculate renal function, and this harrowing story of stillbirth due to the fact transman with abdominal pain was mis-sexed in the ER.
WHAT HAPPENS WHEN A WOMAN ASKS FOR A FEMALE HEALTHCARE PROVIDER
“Had my 1st experience in the 1st lockdown, finally built enough courage to tell my gp why a colonoscopy was such a difficult procedure to subject myself to but was reassured, had a general, came round to a trans identified male nurse pinning me down I was completely freaked out!”
When asked whether she requested a female provider:
“Yes I did because I have urge incontinence and knew if I was out for the count I was going to wet myself and would need changing.”
When told that is not right and asked whether she complained:
“Tbh I thought of nothing else afterwards but I don’t trust the Trust or the NHS not to treat me as the problem and as someone with chronic conditions I don’t need anything else to negatively impact my care.“
ANTENATAL SCREENING
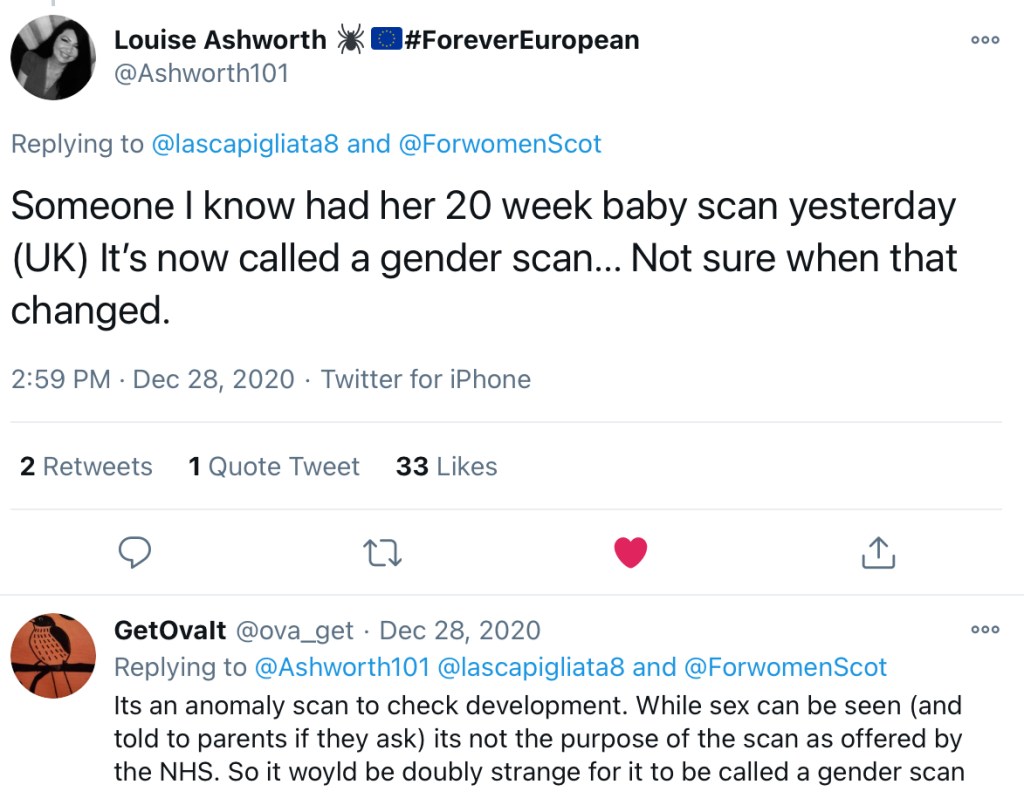
“Someone I know had her 20 week baby scan yesterday (UK) It’s now called a gender scan… Not sure when that changed.”
BREAST CANCER SCREENING
“I was filling out a breast cancer related questionnaire (American) and it asked me what sex I was assigned at birth. The very nice woman who designed it was trying to be kind and inclusive.”

BREAST SURGERY
“[California] moves to change insurance language on double mastectomies for gender dysphoric females from “cosmetic” to “reconstructive” to ensure no age limit for the procedure. Normal breasts are reclassified as “abnormal structures of the body caused by congenital defects.””



TESTOSTERONE PRESCRIPTIONS FOR FEMALE TRANS PATIENTS
“However, transgender men are males, and they have low testosterone levels, so they have androgen deficiency, and they don’t have testicles. So, we’ve been able to use the indication of ‘androgen deficiency due to an established testicular disorder’.”

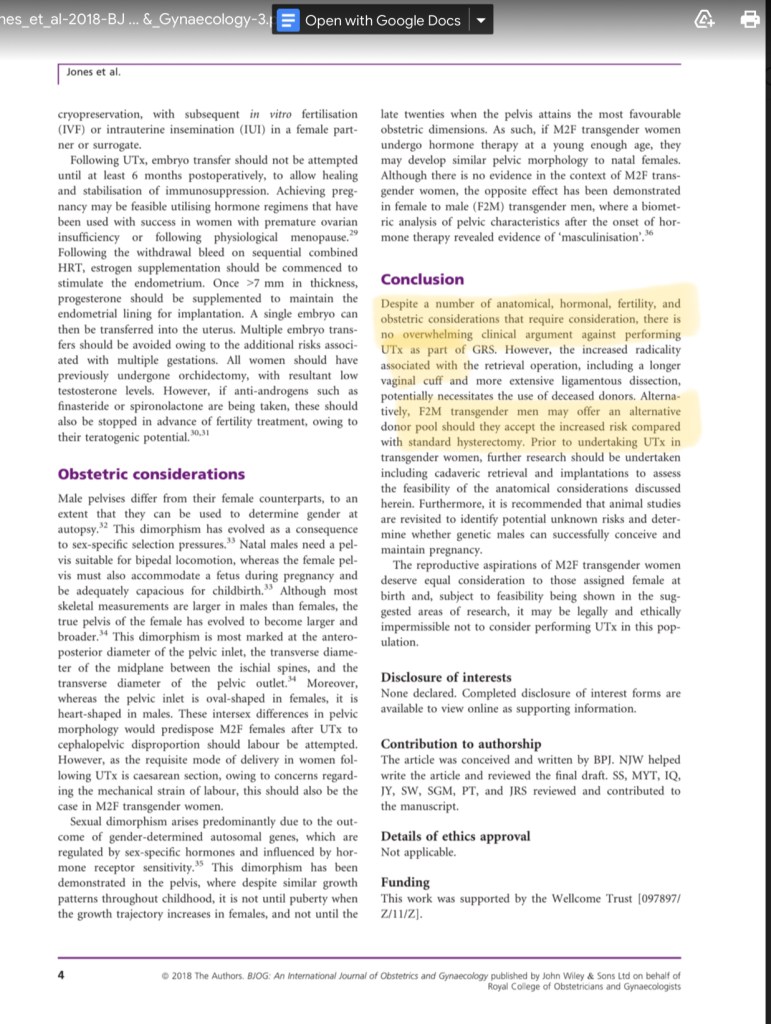
UTERINE IMPLANTS INTO MALE TRANS PATIENTS
Absolute Uterine Factor Infertility is a condition by which women, ie. adult human females, cannot get pregnant due to absence of uterus or uterine dysfunction. Much like in the above case, incorrect language – calling men who “identify as women” actual women – is used to allege that a man gets AUFI the moment he utters the words “I identify as a woman” and it goes on to make an extraordinary claim it would be illegal to *not* offer uterine transplants to these men. Furthermore, a conflict of interest is introduced when transmen are suggested as a potential source of these uteruses.

CERVICAL CANCER SCREENING
Irish cervical screening material now mentions word “woman” but completely omits word “female” which leads to very muddled, borderline misleading statements such as
“Every year in Ireland about 300 people get cervical cancer. 90 women die from it.”
This is despite surveys showing most women don’t know what a cervix is, and that many are unaware of the screening at all.
COVID 19
“Taking part in a Covid antibody research trial. They are not recording sex. They asked – What gender are you? – male, female, Non-binary, other. Really don’t see the point in them asking at all. When they start doing this in medical research, you know the world has gone to shit.”

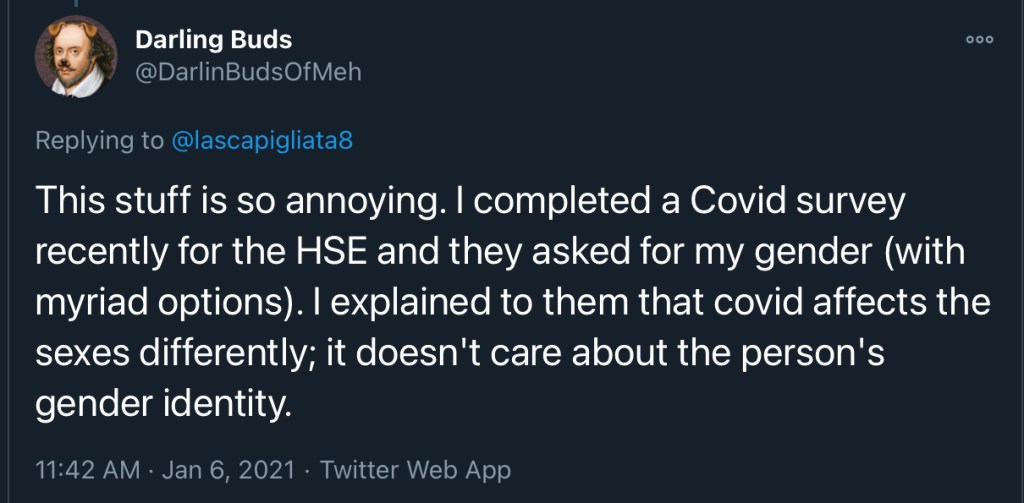
“I completed a Covid survey recently for the HSE and they asked for my gender (with myriad options). I explained to them that covid affects the sexes differently; it doesn’t care about the person’s gender identity.”
“This is what you are asked if you book a COVID test online. Following Q asks race with an explanation of why it’s so important because it helps understand how COVID affects different races.”

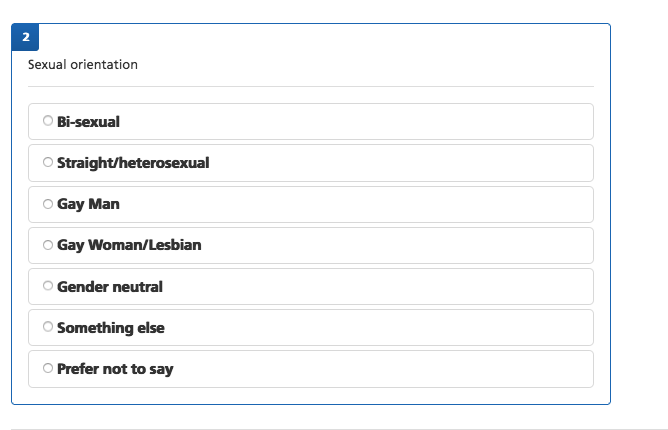
“I’ve recently applied to NHS Professionals to be a COVID vaccinator. The equalities monitoring form I had to sign was bonkers. It firstly asked for my ‘sex assigned at birth’ (using the politicised language of trans activists), rather than just my sex (which is determined at fertilisation and is not ‘assigned’). It then listed ‘intersex’ as one of the options, as if being intersex is a ‘third sex’, when all those with Differences of Sexual Development (DSDs, or ‘intersex’) are either male or female. It then (ridiculously and irrelevantly) asked me for my sexual orientation. Amongst the many options the NHS Professionals included was ‘gender neutral’ as if this is a sexuality! It didn’t inspire much confidence.”

NHS BLOOD AND TRANSPLANT
This one was particularly harrowing considering that men can experience severe adverse reactions from receiving blood and plasma from women and that sex mismatch between donor and recipient can contribute to incresed rejection and complication rates of organ transplant procedures.

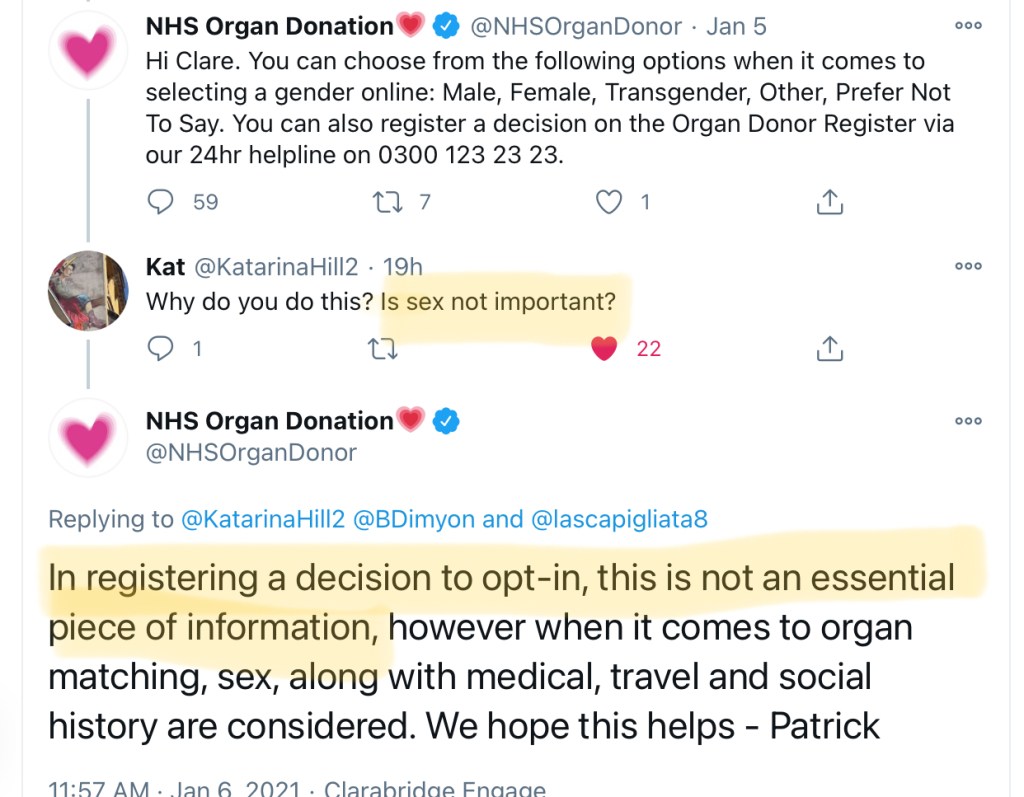
When asked about why they use for “gender” not “sex”:
“You can choose from the following options when it comes to selecting a gender online: Male, Female, Transgender, Other, Prefer Not To Say. You can also register a decision on the Organ Donor Register via our 24hr helpline on 0300 123 23 23.”

When pressed repeatedly about potential for medical errors if gender, rather than sex, are recorded:
“In registering a decision to opt-in, this is not an essential piece of information, however when it comes to organ matching, sex, along with medical, travel and social history are considered. We hope this helps –“
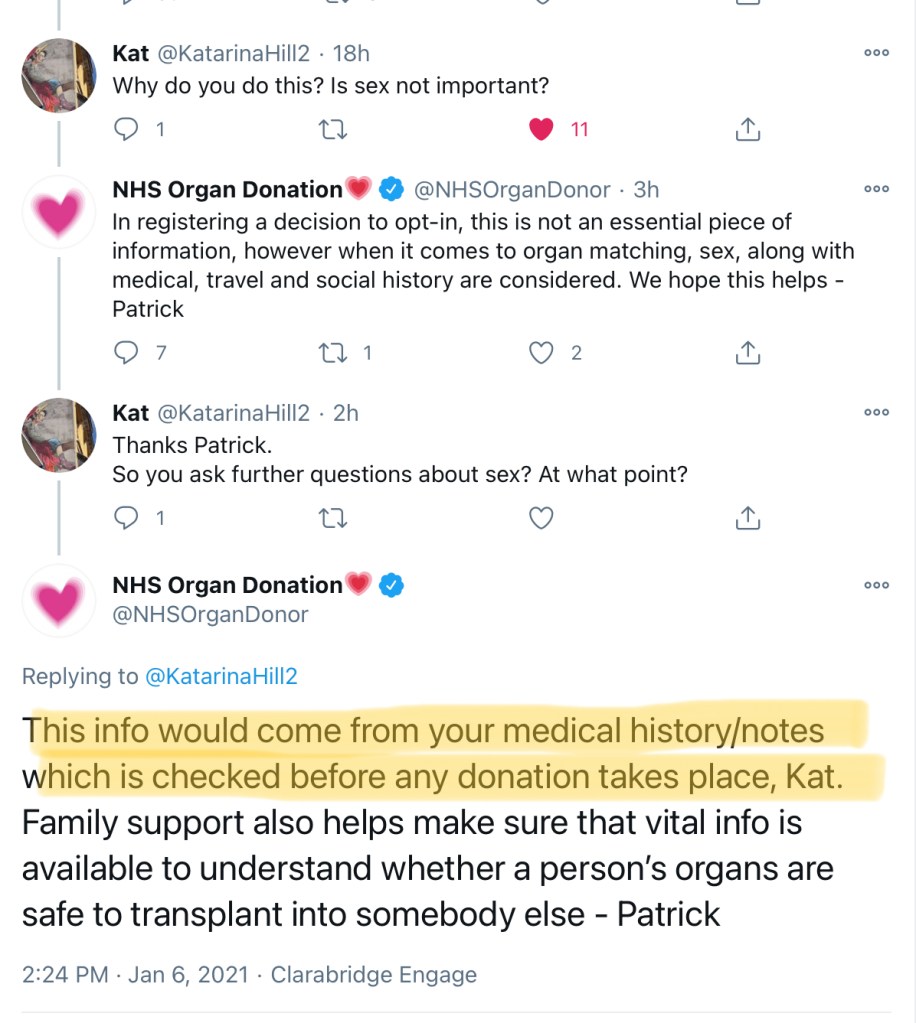
“This info would come from your medical history/notes which is checked before any donation takes place, Kat. Family support also helps make sure that vital info is available to understand whether a person’s organs are safe to transplant into somebody else -“
However, as demonstrated previously, when new record is created, all information relating to patient’s biological sex (erroneously referred to as “gender identity”) is removed from the new record.
There is also an issue of collecting irrelevant information ie. “gender” as opposed to “sex”:
“Specifically the third principle that the information is “used in a way that is adequate, relevant and limited to only what is necessary”.”

“When I opted in years ago, I was told to select my sex. Why is it now different? Nothing has changed between then and now. Women are still female and men are still male. Everything else is personality and makes no difference to their organs.”

I believe this is enough to illustrate the enormity of the problem, and hope this article serves as a call to action.
Medical profession and healthcare of all patients, and especially women and people who identify as transgender, have been severely compromised by allowing ideology to influence medical policies and procedures, and it will take a joint effort of many clinicians, politicians and members of public to put a stop to it.
Having said that, it is unacceptable that the burden of addressing the issue of biology denialism in the medical profession has fallen on patients. The longer medical establishment and individual clinicians remain silent, the more severely compromised doctor-patient relationship and public trust in medical profession will become.

A pal of mine works in organ transplantation with living donors. They have had a transman tick “male” and turn up to donate to a male recipient. It could have gone badly wrong.
LikeLiked by 4 people
Thank you for this comment. That’s dreadful yet not unexpected. This is why doctors must be allowed to enquire, and make their own judgements on patient’s sex and other clinical parameters and to clearly communicate this info in the notes. It’s not safe or appropriate to put patients in charge of what truthful and relevant info doctors can or can’t communicate in clinical settings.
LikeLiked by 3 people
History matters. The space between origin and result matters, not simply the lifelong transformation we all experience, but the history from here to there. It doesn’t matter what you call it, but if you aren’t able to accept facts, then you will never accept yourself, in any form. No one starts out perfect and complete. But we start out with personal differences that must be categorized in order to help you, not to hurt you. Physical and psychological are both important. You have to face medical facts if you want to be a “self-realized” individual. It’s better for the mind to understand reality, and move on from there. Physical reality will exist no matter what you imagine yourself to be, no matter how others see you, or how you think of yourself. It doesn’t matter what you call it. Categories drive medicine. Evolution is a fact. Biology is a fact. That’s not reactionary, it’s actually advanced medicine. And for the mind, I would suggest that to accept oneself, as one is born, regardless of how one behaves, might lead to a better world. But if not, just remember that medical history matters!
LikeLiked by 4 people
Thank you for such an insightful comment Phoebe. Living a life pretending we are something that we are not is stressful. The resulting paranoia, self-checking and allowing our self-esteem to be dependant on reactions and feedback of others, or increasingly, their reluctant, coerced compliance to go along with an obvious lie, cannot be healthy in the long run. Reality matters in so many ways, and biological sex is the most fundamental piece of information a doctor needs when treating a patient. Therefore I think these policies directly compromise doctor’s ability to do their job. However, when everything goes wrong, it will be individual doctors who are blamed for bad outcomes, and these policies won’t matter one iota, it’ll all be on them.
LikeLiked by 2 people
Bravo. Long time reader of your thoughts, this is outstanding.
Advocates of “science based medicine” (who have done a great job at calling out so many pseudoscientific practices) have been spineless throughout al of this and openly aligned with many of the deepest parts of this ideology.
LikeLiked by 3 people
I’ve recently applied to NHS Professionals to be a COVID vaccinator. The equalities monitoring form I had to sign was bonkers. It firstly asked for my ‘sex assigned at birth’ (using the politicised language of trans activists), rather than just my sex (which is determined at fertilisation and is not ‘assigned’). It then listed ‘intersex’ as one of the options, as if being intersex is a ‘third sex’, when all those with Differences of Sexual Development (DSDs, or ‘intersex’) are either male or female. It then (ridiculously and irrelevantly) asked me for my sexual orientation. Amongst the many options the NHS Professionals included was ‘gender neutral’ as if this is a sexuality! It didn’t inspire much confidence. I have screenshots if you want to add them later.
LikeLiked by 3 people
Thanks ffor posting this
LikeLiked by 1 person